| Posttraumatic stress disorder | |
|---|---|
|
File:USMC-120503-M-9426J-001.jpg A mask, painted by a Marine who attended art therapy to relieve posttraumatic stress disorder symptoms | |
| Classification and external resources | |
| ICD-10 | F43.1 |
| ICD-9-CM | 309.81 |
| Diseases Database | 33846 |
| MedlinePlus | 000925 |
| eMedicine | med/1900 |
| MeSH | D013313 |
{kind=link}
Posttraumatic stress disorder[note 1] (PTSD) is a severe condition that may develop after a person is exposed to one or more traumatic events, such as sexual assault, serious injury or the threat of death.[1] The diagnosis may be given when a group of symptoms such as disturbing recurring flashbacks, avoidance or numbing of memories of the event, and hyperarousal (high levels of anxiety) continue for more than a month after the traumatic event.[1]
Most people who experience a traumatizing event will not develop PTSD.[2] Women are more likely to experience more high impact trauma, and are also more likely to develop PTSD than men.[2] Children are less likely to experience PTSD after trauma than adults, especially if they are under 10 years of age.[2] War veterans are commonly at risk to PTSD.
Classification[]
Posttraumatic stress disorder is classified as an anxiety disorder; the characteristic symptoms are not present before exposure to the violently traumatic event. Typically the individual with PTSD persistently avoids all thoughts, emotions and discussion of the stressor event and may experience amnesia for it. However, the event is commonly relived by the individual through intrusive, recurrent recollections, flashbacks and nightmares.[3] The characteristic symptoms are considered acute if lasting less than three months, and chronic if persisting three months or more, and with delayed onset if the symptoms first occur after six months or some years later. PTSD is distinct from the briefer acute stress disorder, and can cause clinical impairment in significant areas of functioning.[4][5][6]
Causes[]

.jpg){kind=link}
No quieren (They do not want to) by Francisco Goya (1746–1828) depicts an elderly woman wielding a knife in defense of a young girl who is being assaulted by a soldier.[7]
PTSD is believed to be caused by the experience of a wide range of traumatic events and, particularly if the trauma is extreme, can occur in persons with no predisposing conditions.[8][9]
Persons considered at risk include combat military personnel, victims of natural disasters, concentration camp survivors and victims of violent crime. Individuals not infrequently experience "survivor's guilt" for remaining alive while others died. Causes of the symptoms of PTSD are the experiencing or witnessing of a stressor event involving death, serious injury or such threat to the self or others in a situation in which the individual felt intense fear, horror, or powerlessness.[10] Persons who are employed in occupations which expose them to violence (such as soldiers) or disasters (such as emergency service workers) are also at risk.[10]
Children or adults may develop PTSD symptoms by experiencing bullying or mobbing.[11][12]
Family violence[]
Trauma from family violence can predispose an individual to PTSD. Approximately 25% of children exposed to family violence can experience PTSD in a study of 337 school age children.[13] Preliminary research suggests that child abuse may interact with mutations in a stress-related gene to increase the risk of PTSD in adults, in a cross-sectional study of 900 school age children.[14][15][16] However, being exposed to a traumatic experience doesn't automatically indicate they will develop PTSD.[17] It has been shown that the intrusive memories, such as flashbacks, nightmares, and the memories themselves, are greater contributors to the biological and psychological dimensions of PTSD than the event itself.[18] These intrusive memories are mainly characterized by sensory episodes, rather than thoughts. People with PTSD have intrusive re-experiences of traumatic events which lack awareness of context and time. These episodes aggravate and maintain PTSD symptoms since the individual re-experiences trauma as if it was happening in the present moment.[19]
Multiple studies show that parental PTSD and other posttraumatic disturbances in parental psychological functioning can, despite a traumatized parent's best efforts, interfere with their response to their child as well as their child's response to trauma. For example, in two studies by Schechter, one of 67 mothers and another of 25 mothers, this was shown to be the case.[20][21] Parents with violence-related PTSD may, for example, inadvertently expose their children to developmentally inappropriate violent media due to their need to manage their own emotional dysregulation.[22] Clinical findings indicate that a failure to provide adequate treatment to children after they suffer a traumatic experience, depending on their vulnerability and the severity of the trauma, will ultimately lead to PTSD symptoms in adulthood.[23]
Evolutionary psychology[]
Evolutionary psychology views different types of fears and reactions caused by fears as adaptations that may have been useful in the ancestral environment in order to avoid or cope with various threats. Mammals generally display several defensive behaviors roughly dependent on how close the threat is: avoidance, vigilant immobility, withdrawal, aggressive defense, appeasement, and finally complete frozen immobility (the last possibly to confuse a predator's attack reflex or to simulate a dead and contaminated body). PTSD may correspond to and be caused by overactivation of such fear circuits. Thus, PTSD avoidance behaviors may correspond to mammal avoidance of and withdrawal from threats. Heightened memory of past threats may increase avoidance of similar situations in the future as well as be a prerequisite for analyzing the past threat and develop better defensive behaviors if the threat should recur. PTSD hyperarousal may correspond to vigilant immobility and aggressive defense. Complex posttraumatic stress disorder (and phenomena such as the Stockholm syndrome) may in part correspond to the appeasement stage and possibly the frozen immobility stage.[24][25]
There may be evolutionary explanations for differences in resilience to traumatic events. Thus, PTSD is rare following traumatic fire which may be explained by events such as forest fires long being part of the evolutionary history of mammals. On the other hand, PTSD is much more common following modern warfare, which may be explained by modern warfare being a new development and very unlike the quick inter-group raids that are argued to have characterized the paleolithic.[26]
Genetics[]
There is evidence that susceptibility to PTSD is hereditary. Approximately 30% of the variance in PTSD is caused from genetics alone. For twin pairs exposed to combat in Vietnam, having a monozygotic (identical) twin with PTSD was associated with an increased risk of the co-twin having PTSD compared to twins that were dizygotic (non-identical twins).[27] There is also evidence that those with a genetically smaller hippocampus are more likely to develop PTSD following a traumatic event. Research has also found that PTSD shares many genetic influences common to other psychiatric disorders. Panic and generalized anxiety disorders and PTSD share 60% of the same genetic variance. Alcohol, nicotine, and drug dependence shares greater than 40% genetic similarities.[28]
Gamma-aminobutyric acid (GABA) is the major inhibitory neurotransmitter in the brain. A recent study reported significant interactions between three polymorphisms in the GABA alpha-2 receptor gene and the severity of childhood trauma in predicting PTSD in adults. A study found those with a specific genotype for G-protein signaling 2 (RGS2), a protein that decreases G protein-coupled receptor signaling, and high environmental stress exposure as adults and a diagnosis of lifetime PTSD. This was particularly prevalent in adults with prior trauma exposure and low social support.[28]
Recently, it has been found that several single-nucleotide polymorphisms (SNPs) in FK506 binding protein 5 (FKBP5) interact with childhood trauma to predict severity of adult PTSD.[29][30] These findings suggest that individuals with these SNPs who are abused as children are more susceptible to PTSD as adults.
This is particularly interesting given that FKBP5 SNPs have previously been associated with peritraumatic dissociation in a study of polymorphisms in FKBP5 associated with peritraumatic dissociation in medically injured children (that is, dissociation at the time of the birth trauma),[31] which has itself been shown to be predictive of PTSD.[32][33] Furthermore, FKBP5 may be less expressed in those with current PTSD.[34] Another recent study found a single SNP in a putative estrogen response element on ADCYAP1R1 (encodes pituitary adenylate cyclase-activating polypeptide type I receptor or PAC1) to predict PTSD diagnosis and symptoms in females.[35] Incidentally, this SNP is also associated with fear discrimination. The study suggests that perturbations in the PACAP-PAC1 pathway are involved in abnormal stress responses underlying PTSD.
PTSD is a psychiatric disorder which requires an environmental event which individuals may have varied responses to so gene-environment studies tend to be the most indicative of their effect on the probability of PTSD then studies of the main effect of the gene. Recent studies have demonstrated the interaction between PFBP5 and childhood environment to predict the severity of PTSD. Polymorphisms in FKBP5 have been associated with peritraumatic dissociation in mentally ill children. A study of highly traumatized African-American subjects from inner city primary care clinics indicated 4 polymorphisms of the FKBP5 gene, each of these were functional. The interaction between the polymorphisms and the severity of childhood abuse predicts the severity of the adult PTSD symptoms. A more recent study of the African-American population indicated that the TT genotype of the FKBP5 gene was associated with the highest risk of PTSD among those who experienced childhood adversity, however those with this genotype that experienced no childhood adversity had the lowest risk of PTSD. In addition alcohol dependence interacts with the FKBP5 polymorphisms and childhood adversity to increase the risk of PTSD in these populations. Emergency room expression of the FKPB5 mRNA following trauma was shown to indicate a later development of PTSD.[28]
Catechol-O-methyl transferase (COMT) is an enzyme that catalyzes the extraneuronal breakdown of catecholamines. The gene that codes for COMT has a functional polymorphism in which a valine has been replaced with a methionine at codon 158. This polymorphism has lower enzyme activity and has been tied to slower breakdown of the catecholamines. A study, of Rwandan Genocide survivors, indicated that carriers of the Val allel demonstrated the expected response relationship between the higher number of lifetime traumatic events and a lifetime diagnosis of PTSD. However those who were homozygotes for the Met/Met genotype demonstrated a high risk of lifetime PTSD independent of the number of traumatic experiences. Those with Met/Met genotype also demonstrated a reduced extinction of conditioned fear responses with may account for the high risk for PTSD experienced by this genotype.[28]
Many genes impact the limbic-frontal neurocircuitry as a result of its complexity. The main effect of the D2A1 allele of the dopamine receptor D2 (DRD2) has a strong association with the diagnosis of PTSD. The D2A1 allele has also shown a significant association to PTSD in those who engaged in harmful drinking. In addition a polymorphism in the dopamine transporter SLC6A3 gene has a significant association with chronic PTSD. A polymorphism of the serotonin receptor 2A gene has been associated with PTSD in Korean women. The short allele of the promoter region of the serotonin transporter (5-HTTLPR) has been shown to be less efficient then the long allele and is associated with the amygdala response for extinction of fear conditioning. However the short allele is associated with a decreased risk of PTSD in a low risk environment but a high risk of PTSD in a high risk environment. The s/s genotype demonstrated a high risk for development of PTSD even in response to a small number of traumatic events but those with the l allele demonstrate increasing rates of PTSD with increasing traumatic experiences.[28]
Genome-wide association study (GWAS) offer an opportunity to identify novel risk variants for PTSD which will in turn inform our understanding of the etiology of the disorder. Early results indicate the feasibility and potential power of GWAS to identify biomarkers for anxiety-related behaviors that suggest a future of PTSD. These studies will lead to the discovery of novel loci for the susceptibility and symptomatology of anxiety disorders including PTSD.[28]
Epigenetics[]
Gene and environment studies alone fail to explain the importance the developmental stressor timing exposure to the phenotypic changes associated with PTSD. Epigenetic modification is the environmentally induced change in DNA which alters the function rather than the structure of the gene. The biological mechanism of epigenetic modification typically involves the methylation of cytosine within a gene which produces decreased transcription of that segment of DNA. The neuroendocrine alteration seen in animal models parallel those of PTSD in which low basal cortisol and enhanced suppression of cortisol in response to synthetic glucocorticoid becomes hereditary. Lower levels of glucocorticoid receptor (GR) mRNA have been demonstrated in the hippocampus of suicide victims with histories of childhood abuse. It hasn’t been possible to monitor the state of methylation over time however the interpretation is early developmental methylation changes are long-lasting and enduring. It is hypothesized that epigenetic-mediated changes in the HPA axis could be associated with an increased vulnerability to PTSD following traumatic events. These findings support the mechanism in which early life trauma strongly validates as a risk factor for PTSD development in adulthood by recalibrating the set point and stress-responsivity of the HPA axis. Studies have reported an increased risk for PTSD and low cortisol levels in the offspring of female holocaust survivors with PTSD. Epigenetic mechanisms may also be relevant to the intrauterine environment. Mothers with PTSD produced infants with lower salivary cortisol levels only if the traumatic exposure occurred during the third trimester of gestation. These changes occur via transmission of hormonal responses to the fetus leading to a reprogramming of the glucocorticoid responsivity in the offspring.[28]
Risk factors[]
Most people (more than half) will experience at least one traumatizing event in their lifetime.[36] Men are more likely to experience a traumatic event, but women are more likely to experience the kind of high impact traumatic event that can lead to PTSD, such as interpersonal violence and sexual assault.[2] Only a minority of people who are traumatized will develop PTSD, but they are more likely to be women. The average risk of developing PTSD after trauma is around 8% for men, while for women it is just over 20%.[2] The risk is believed to be higher in young urban populations (24%): 13% for men and 30% for women.[2] Rates of PTSD are higher in combat veterans than other men, with a rate estimated at up to 20% for veterans returning from Iraq and Afghanistan.[36]
Posttraumatic stress reactions have not been studied as well in children and adolescents as adults.[2] The rate of PTSD may be lower in children than adults, but in the absence of therapy, symptoms may continue for decades.[2] One estimate suggests that the proportion of children and adolescents having PTSD in a non-wartorn population in a developed country may be 1% compared to 1.5% to 3% of adults, and much lower below the age of 10 years.[2]
Predictor models have consistently found that childhood trauma, chronic adversity, and familial stressors increase risk for PTSD as well as risk for biological markers of risk for PTSD after a traumatic event in adulthood.[37][38][39][40] Peritraumatic dissociation in children is a predictive indicator of the development of PTSD later in life.[28] This effect of childhood trauma, which is not well understood, may be a marker for both traumatic experiences and attachment problems.[41][42] Proximity to, duration of, and severity of the trauma also make an impact, and interpersonal traumas cause more problems than impersonal ones.[43]
Quasi-experimental studies have demonstrated a relationship between intrusive thoughts and intentional control responses such that suppression increases the frequency of unwanted intrusive thoughts. These results suggest that suppression of intrusive thoughts may be important in the development and maintenance of PTSD.[44]
Military experience[]
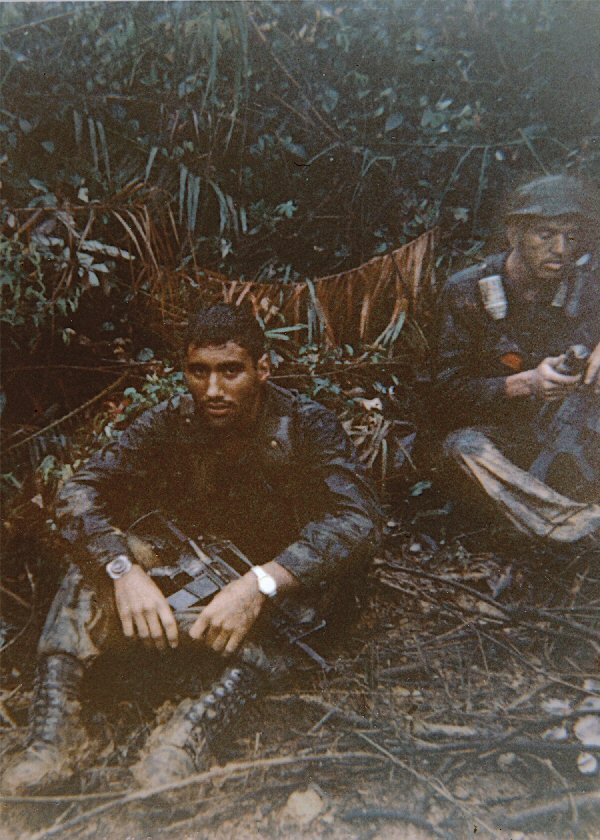
{kind=link}
A U.S. Long Range Reconnaissance Patrol team leader in Vietnam, 1968.
Schnurr, Lunney, and Sengupta[33] identified risk factors for the development of PTSD in Vietnam veterans. The subjects were 68 women and 414 men of whom 88 were white, 63 black, 80 Hispanic, 90 Native Hawaiian, and 93 Japanese American. Among their findings were:
- Hispanic ethnicity, coming from an unstable family, being punished severely during childhood, childhood asocial behavior, and depression as pre-military factors
- War-zone exposure, peritraumatic dissociation, depression as military factors
- Recent stressful life events, post-Vietnam trauma, and depression as post-military factors
They also identified certain protective factors, such as:
- Japanese-American ethnicity, high school degree or college education, older age at entry to war, higher socioeconomic status, and a more positive paternal relationship as pre-military protective factors
- Social support at homecoming and current social support as post-military factors.[45] Other research also indicates the protective effects of social support in averting PTSD or facilitating recovery if it develops.[46][47]
Glass and Jones found early intervention to be a critical preventive measure:
"PTSD symptoms can follow any serious psychological trauma, such as exposure to combat, accidents, torture, disasters, criminal assault and exposure to atrocities or to the sequelae of such extraordinary events. Prisoners of war exposed to harsh treatment are particularly prone to develop PTSD. In their acute presentation these symptoms, which include subsets of a large variety of affective, cognitive, perceptional, emotional and behavioral responses which are relatively normal responses to gross psychological trauma. If persistent, however, they develop a life of their own and may be maintained by inadvertent reinforcement. Early intervention and later avoidance of positive reinforcement (which may be subtle) for such symptoms is a critical preventive measure.[48]
Studies have shown that those prepared for the potential of a traumatic experience are more prepared to deal with the stress of a traumatic experience and therefore less likely to develop PTSD.[49]
Drug misuse[]
Alcohol abuse and drug abuse commonly co-occur with PTSD.[50] Recovery from posttraumatic stress disorder or other anxiety disorders may be hindered, or the condition worsened, by medication or substance overuse, abuse, or dependence; resolving these problems can bring about a marked improvement in an individual's mental health status and anxiety levels.[51][52]
Yohimbine (not considered specifically appropriate for PTSD) increases arousal by increasing release of endogenous norepinephrine and can worsen PTSD symptoms.[50][Clarification needed]
Foster care[]
In the Casey Family Northwest Alumni Study, conducted in conjunction with researchers from the Harvard Medical School in Oregon and Washington state, the rate of PTSD in adults who were in foster care for one year between the ages of 14–18 was found to be higher than that of combat veterans. Up to 25% of those in the study meet the diagnostic criteria for PTSD as compared to 12–13% of Iraq war veterans and 15% of Vietnam War veterans, and a rate of 4% in the general population. The recovery rate for foster home alumni was 28.2% as opposed to 47% in the general population.[53][54]
Dubner and Motta (1999)[55] found that 60% of children in foster care who had experienced sexual abuse had PTSD, and 42% of those who had been physically abused met the PTSD criteria. PTSD was also found in 18% of the children who were not abused. These children may have developed PTSD due to witnessing violence in the home, or as a result of real or perceived parental abandonment.
Pathophysiology[]
Neuroendocrinology[]
PTSD symptoms may result when a traumatic event causes an over-reactive adrenaline response, which creates deep neurological patterns in the brain. These patterns can persist long after the event that triggered the fear, making an individual hyper-responsive to future fearful situations.[49][56] During traumatic experiences the high levels of stress hormones secreted suppress hypothalamic activity which may be a major factor towards the development of PTSD.[57]
PTSD causes biochemical changes in the brain and body that differ from other psychiatric disorders such as major depression. Individuals diagnosed with PTSD respond more strongly to a dexamethasone suppression test than individuals diagnosed with clinical depression.[58][59]
In addition, most people with PTSD also show a low secretion of cortisol and high secretion of catecholamines in urine,[60] with a norepinephrine/cortisol ratio consequently higher than comparable non-diagnosed individuals.[61] This is in contrast to the normative fight-or-flight response, in which both catecholamine and cortisol levels are elevated after exposure to a stressor.[62]
Brain catecholamine levels are high,[63] and corticotropin-releasing factor (CRF) concentrations are high.[64][65] Together, these findings suggest abnormality in the hypothalamic-pituitary-adrenal (HPA) axis.
The HPA axis is responsible for coordinating the hormonal response to stress.[28] Given the strong cortisol suppression to dexamethasone in PTSD, HPA axis abnormalities are likely predicated on strong negative feedback inhibition of cortisol, itself likely due to an increased sensitivity of glucocorticoid receptors.[66] Some researchers have associated the response to stress in PTSD with long-term exposure to high levels of norepinephrine and low levels of cortisol, a pattern associated with improved learning in animals.[citation needed]
Translating this reaction to human conditions gives a pathophysiological explanation for PTSD by a maladaptive learning pathway to fear response through a hypersensitive, hyperreactive, and hyperresponsive HPA axis.[67]
Low cortisol levels may predispose individuals to PTSD: Following war trauma, Swedish soldiers serving in Bosnia and Herzegovina with low pre-service salivary cortisol levels had a higher risk of reacting with PTSD symptoms, following war trauma, than soldiers with normal pre-service levels.[68] Because cortisol is normally important in restoring homeostasis after the stress response, it is thought that trauma survivors with low cortisol experience a poorly contained—that is, longer and more distressing—response, setting the stage for PTSD.
Other studies indicate that people that suffer from PTSD have chronically low levels of serotonin which contributes to the commonly associated behavioral symptoms such as anxiety, ruminations, irritability, aggression, suicidality, and impulsivity.[18] Serotonin also contributes to the stabilization of glucocorticoid production.
Dopamine levels in patients with PTSD can help contribute to the symptoms associated. Low levels of dopamine can contribute to anhedonia, apathy, impaired attention, and motor deficits. Increased levels of dopamine can cause psychosis, agitation, and restlessness.[18]
Hyperresponsiveness in the norepinephrine system can be caused by continued exposure to high stress. Overactivation of norepinephrine receptors in the prefrontal cortex can be connected to the flashbacks and nightmares frequently experienced by those with PTSD. A decrease in other norepinephrine functions (awareness of the current environment) prevents the memory mechanisms in the brain from processing that the experience, and emotions the person is experiencing during a flashback are not associated with the current environment.[18]
However, there is considerable controversy within the medical community regarding the neurobiology of PTSD. A review of existing studies on this subject showed no clear relationship between cortisol levels and PTSD. However the majority of reports indicate people with PTSD have elevated levels of corticotropin-releasing hormone, lower basal cortisol levels, and enhanced negative feedback suppression of the HPA axis by dexamethasone.[28][69]
Neuroanatomy[]
{kind=link}
Regions of the brain associated with stress and posttraumatic stress disorder[70]
Three areas of the brain in which function may be altered in PTSD have been identified: the prefrontal cortex, amygdala, and hippocampus. Much of this research has utilised PTSD victims from the Vietnam War. For example, a prospective study using the Vietnam Head Injury Study showed that damage to the prefrontal cortex may actually be protective against later development of PTSD.[71] In a study by Gurvits et al., combat veterans of the Vietnam War with PTSD showed a 20% reduction in the volume of their hippocampus compared with veterans who suffered no such symptoms.[72] This finding could not be replicated in chronic PTSD patients traumatized at an air show plane crash in 1988 (Ramstein, Germany).[73][74]
In human studies, the amygdala has been shown to be strongly involved in the formation of emotional memories, especially fear-related memories. Neuroimaging studies in humans have revealed both morphological and functional aspects of PTSD.[75] However during high stress times the hippocampus, which is associated with the ability to place memories in the correct context of space and time, and with the ability to recall the memory, is suppressed. This suppression is hypothesized to be the cause of the flashbacks that often plague PTSD patients. When someone with PTSD undergoes stimuli similar to the traumatic event the body perceives the event as occurring again because the memory was never properly recorded in the patients memory.[28]
The amygdalocentric model of PTSD proposes that it is associated with hyperarousal of the amygdala and insufficient top-down control by the medial prefrontal cortex and the hippocampus particularly during extinction.[76] This is consistent with an interpretation of PTSD as a syndrome of deficient extinction ability.[76][77] A study at the European Neuroscience Institute-Goettingen (Germany) found that fear extinction-induced IGF2/IGFBP7 signalling promotes the survival of 17–19-day-old newborn hippocampal neurons. This suggests that therapeutic strategies that enhance IGF2 signalling and adult neurogenesis might be suitable to treat diseases linked to excessive fear memory such as PTSD.[78] Further animal and clinical research into the amygdala and fear conditioning may suggest additional treatments for the condition.
The maintenance of the fear involved with PTSD has been shown to include the HPA axis, the locus coeruleus-noradrenergic systems, and the connections between the limbic system and frontal cortex. The HPA axis which coordinates the hormonal response to stress[79] which activates the LC-noradrenergic system is implicated in the over consolidation of memories that occurs in the aftermath of trauma.[80] This over consolidation increases the likelihood of developing PTSD. The amygdala is responsible for threat detection and the conditioned and unconditioned fear responses that are carried out as a response to a threat.[28]
The LC-noradrenergic system has been hypothesized to mediate the over-consolidation of fear memory in PTSD. High levels of cortisol reduces noradrenergic activity it is proposed that individuals with PTSD fail to regulate the increased noradrenergic response to traumatic stress.[81][Clarification needed] It is thought that the intrusive memories and conditioned fear responses to associated triggers is a result of this response. Neuropeptide Y has been reported to reduce the release of norepinephrine and has been demonstrated to have anxiolytic properties in animal models. Studies have shown people with PTSD demonstrate reduced levels of NPY, possibly indicating their increased anxiety levels.[28]
The basolateral nucleus (BLA) of the amygdala is responsible for the comparison and development of associations between unconditioned and conditioned responses to stimuli which results in the fear conditioning present in PTSD. The BLA activates the central nucleus (CeA) of the amygdala which elaborates the fear response, (including behavioral response to threat and elevated startle response). Descending inhibitory inputs from the medial prefrontal cortex (mPFC) regulate the transmission from the BLA to the CeA which is hypothesized to play a role in the extinction of conditioned fear responses.[28]
Diagnosis[]
Diagnostic and Statistical Manual[]
The diagnostic criteria for PTSD, stipulated in the Diagnostic and Statistical Manual of Mental Disorders IV (Text Revision) (DSM-IV-TR), may be summarized as:[3][82]
A: Exposure to a traumatic event. This must have involved both (a) loss of "physical integrity", or risk of serious injury or death, to self or others, and (b) a response to the event that involved intense fear, horror, or helplessness (or in children, the response must involve disorganized or agitated behavior). (The DSM-IV-TR criterion differs substantially from the previous DSM-III-R stressor criterion, which specified the traumatic event should be of a type that would cause "significant symptoms of distress in almost anyone," and that the event was "outside the range of usual human experience."[83])
B: Persistent re-experiencing. One or more of these must be present in the victim: flashback memories, recurring distressing dreams, subjective re-experiencing of the traumatic event(s), or intense negative psychological or physiological response to any objective or subjective reminder of the traumatic event(s).
C: Persistent avoidance and emotional numbing. This involves a sufficient level of:
- avoidance of stimuli associated with the trauma, such as certain thoughts or feelings, or talking about the event(s);
- avoidance of behaviors, places, or people that might lead to distressing memories as well as the disturbing memories, dreams, flashbacks, and intense psychological or physiological distress;[18]
- inability to recall major parts of the trauma(s), or decreased involvement in significant life activities;
- decreased capacity (down to complete inability) to feel certain feelings;
- an expectation that one's future will be somehow constrained in ways not normal to other people.
D: Persistent symptoms of increased arousal not present before. These are all physiological response issues, such as difficulty falling or staying asleep, or problems with anger, concentration, or hypervigilance. Additional symptoms include irritability, angry outbursts, increased startle response, and concentration or sleep problems.[18]
E: Duration of symptoms for more than 1 month. If all other criteria are present, but 30 days have not elapsed, the individual is diagnosed with Acute stress disorder.[18]
F: Significant impairment. The symptoms reported must lead to "clinically significant distress or impairment" of major domains of life activity, such as social relations, occupational activities, or other "important areas of functioning".[84]
Assessment[]
Since the introduction of DSM-IV, the number of possible events which might be used to diagnose PTSD has increased; one study suggests that the increase is around 50%.[85] Various scales exist to measure the severity and frequency of PTSD symptoms.[86][87] Standardized screening tools such as Trauma Screening Questionnaire[88] and PTSD Symptom Scale[89] can be used to detect possible symptoms of posttraumatic stress disorder and suggest the need for a formal diagnostic assessment.
DSM-5[]
In DSM-5, published in May, 2013, PTSD is classified as a trauma- and stress-related disorder.[1]
- Criterion A: (applicable to adults, adolescents and children over 6. There is a separate Posttraumatic stress disorder for children 6 years and younger.) Exposure to real or threatened death, injury, or sexual violence.
- Several items in Criterion B (intrusion symptoms) are rewritten to add or augment certain distinctions now considered important.
- Special consideration is given to developmentally appropriate criteria for use with children and adolescents. This is especially evident in the restated Criterion B—intrusion symptoms. Development of age-specific criteria for diagnosis of PTSD is ongoing at this time.
- Criterion C (avoidance and numbing) has been split into "C" and "D":
- Criterion C (new version) now focuses solely on avoidance of behaviors or physical or temporal reminders of the traumatic experience(s). What were formerly two symptoms are now three, due to slight changes in descriptions.
- New Criterion D focuses on negative alterations in cognition and mood associated with the traumatic event(s) and contains two new symptoms, one expanded symptom, and four largely unchanged symptoms specified in the previous criteria.
- Criterion E (formerly "D"), which focuses on increased arousal and reactivity, contains one modestly revised, one entirely new, and four unchanged symptoms.
- Criterion F (formerly "E") still requires duration of symptoms to have been at least one month.
- Criterion G (formerly "F") stipulates symptom impact ("disturbance") in the same way as before.
- Criterion H stipulated the disturbance is not due to the effects of a substance or another medical condition.
- Specify whether:
- With dissociative symptoms: (not due to effects of a substance or another medical condition)
- In addition, meets the criteria of Depersonalization
- In addition, meets the criteria of Derealization
- With dissociative symptoms: (not due to effects of a substance or another medical condition)
- Specify if:
- With delayed expression Full criteria not met until more than 6 months after the event
Research-based groups[]
Emerging factor analytic research[90] suggests that PTSD symptoms group empirically into four clusters, not the three currently described in the Diagnostic and Statistical Manual of Mental Disorders[dated info]. One model supported by this research divides the traditional avoidance symptoms into a cluster of numbing symptoms (such as loss of interest and feeling emotionally numb) and a cluster of behavioral avoidance symptoms (such as avoiding reminders of the trauma).[91] An alternative model adds a fourth cluster of dysphoric symptoms. These include symptoms of emotional numbing, as well as anger, sleep disturbance, and difficulty concentrating (traditionally grouped under the hyperarousal cluster).[92][93] A literature review[94] and meta-analysis[95] did not find strong support across the literature for one of these models over the other.
International Classification of Diseases[]
The diagnostic criteria for PTSD, stipulated in the International Statistical Classification of Diseases and Related Health Problems 10 (ICD-10), may be summarized as:[96]
- Exposure to a stressful event or situation (either short or long lasting) of exceptionally threatening or catastrophic nature, which is likely to cause pervasive distress in almost anyone.
- Persistent remembering or "reliving" the stressor by intrusive flash backs, vivid memories, recurring dreams, or by experiencing distress when exposed to circumstances resembling or associated with the stressor.
- Actual or preferred avoidance of circumstances resembling or associated with the stressor (not present before exposure to the stressor).
- Either (1) or (2):
- Inability to recall, either partially or completely, some important aspects of the period of exposure to the stressor
- Persistent symptoms of increased psychological sensitivity and arousal (not present before exposure to the stressor) shown by any two of the following:
- difficulty in falling or staying asleep;
- irritability or outbursts of anger;
- difficulty in concentrating;
- hyper-vigilance;
- exaggerated startle response
The International Statistical Classification of Diseases and Related Health Problems 10 diagnostic guidelines state:[96] This disorder should not generally be diagnosed unless there is evidence that it arose within 6 months of a traumatic event of exceptional severity. A "probable" diagnosis might still be possible if the delay between the event and the onset was longer than 6 months, provided that the clinical manifestations are typical and no alternative identification of the disorder (e.g. as an anxiety or obsessive-compulsive disorder or depressive episode) is plausible. In addition to evidence of trauma, there must be a repetitive, intrusive recollection or re-enactment of the event in memories, daytime imagery, or dreams. Conspicuous emotional detachment, numbing of feeling, and avoidance of stimuli that might arouse recollection of the trauma are often present but are not essential for the diagnosis. The autonomic disturbances, mood disorder, and behavioural abnormalities all contribute to the diagnosis but are not of prime importance. The late chronic sequelae of devastating stress, i.e. those manifest decades after the stressful experience, should be classified under F62.0.
Differential diagnosis[]
A diagnosis of PTSD requires exposure to an extreme stressor such as one that is life-threatening. Any stressor can result in a diagnosis of adjustment disorder and it is an appropriate diagnosis for a stressor and a symptom pattern that does not meet the criteria for PTSD, for example a stressor like a partner being fired, or a spouse leaving. If any of the symptom pattern is present before the stressor, another diagnosis is required, such as brief psychotic disorder or major depressive disorder. Other differential diagnoses are schizophrenia or other disorders with psychotic features such as Psychotic disorders due to a general medical condition. Drug-induced psychotic disorders can be considered if substance abuse is involved.[3]
The symptom pattern for acute stress disorder must occur and be resolved within four weeks of the trauma. If it lasts longer, and the symptom pattern fits that characteristic of PTSD, the diagnosis may be changed.[3]
Obsessive compulsive disorder may be diagnosed for intrusive thoughts that are recurring but not related to a specific traumatic event.[3]
Malingering should be considered if a financial and/or legal advantage is a possibility.
Prevention[]
Modest benefits have been seen from early access to cognitive behavioral therapy, as well as from some medications such as propranolol.[97] Critical incident stress management has been suggested as a means of preventing PTSD, but subsequent studies suggest the likelihood of its producing iatrogenic outcomes.[98][99] A review "...did not find any evidence to support the use of an intervention offered to everyone", and that "...multiple session interventions may result in worse outcome than no intervention for some individuals.[100] The World Health Organization recommends against the use of benzodiazepines and antidepressants in those who have experienced trauma.[101]
Early detection[]
The ability to prescreen individuals would be of great help in getting treatment to those who are at risk of PTSD prior to development of the syndrome. Several biological indicators have been identified that are related to later PTSD development. First, Delhanty[102] found that higher response times and a smaller hippocampal volume were identified as linked to later PTSD development. However, both of these indicators are relatively difficult to test for and need specialized tests or equipment, or both, to identify. A blood biomarker is much easier to test for. Van Zuiden et al.[103] found a biomarker when testing U.S. Army soldiers prior to deployment. They found that soldiers with more glucocorticoid receptors (GR) were more likely to be diagnosed with PTSD six months after deployment. However, higher GR levels have not been identified as a cause of PTSD, and may instead be an intermediator, or even an indicator that the individual has previously experienced traumatic events. There is a great deal of overlap between high GR levels and those who later are diagnosed with and without PTSD. Thus, the identification of high GR is simply a vulnerability indicator at this time.
Delhanty[102] found that biological precursors existed directly following traumatic exposure in those who later developed chronic PTSD and were significantly different from those who did not. Directly following the traumatic event later sufferers often have significantly lower levels of hypothalamic pituitary-adrenal activity and a corresponding decrease in Cortisol. Other methods of early detection include the identification of specific risk factors associated with later PTSD symptoms. Resnick, Acierno, Holmes, Kilpatrick, and Jager[104] for example were able to identify that the forensic exam given to victims after a rape was associated with PTSD. Finally, global treatments attempt to avoid the problems of early detection by simply treating everyone involved. However, many studies[102] have found this to be often ineffective and for global treatments to at times increase prevalence rates of PTSD. Stepped collaborative care is where individuals who are at risk are monitored for symptoms.[97] As symptoms of PTSD appear the level of care is increased to treat those symptoms.
Psychological debriefing[]
The first form of preventive treatment is that of a psychological debriefing.[97] Psychological debriefing is the most often used preventive measure. One of the main reasons for this is the relative ease with which this treatment can be given to individuals directly following an event. It consists of interviews that are meant to allow individuals to directly confront the event and share their feelings with the counselor and to help structure their memories of the event. However, while this form of therapy is the most often used it is the least effective.[97] Studies have had mixed findings concerning psychological debriefings and have ranged from being of significant help to helping in the formation of PTSD in individuals who would otherwise have not developed PTSD.[79] Several meta-analyses have been published, including by the Cochrane Collaboration. They all concluded psychological debriefing is unhelpful and potentially harmful.[105][106] The first Cochrane meta-analysis concerned single-session debriefing. More recently a Cochrane review on multiple session interventions was conducted and also found negative results.[107] The American Psychological Association judges the status of psychological debriefing as No Research Support/Treatment is Potentially Harmful.[108]
Risk targeted interventions[]
Risk targeted interventions are those that attempt to mitigate specific formative information or events. It can target modeling normal behaviors, instruction on a task, or giving information on the event. For example,[104] rape victims were given an instruction video on the procedures for a forensic exam. Also included in the video was advice on how to identify and stop avoidance behavior and control anxiety. Finally, the individuals modeling the forensic exam were shown to be calm and relaxed. PTSD diagnosis for those who saw the video were thirty three percent less than for those who went through the standard forensic procedure.
Medications[]
Some medications have shown benefit in preventing PTSD or reducing its incidence, when given in close proximity to a traumatic event. These medications include:
Alpha-adrenergic agonists. Anecdotal report of success in using clonidine ("Catapres") to reduce traumatic stress symptoms[109] suggests that it may have benefit in preventing PTSD.
Beta blockers. Propranolol ("Inderal"), similarly to clonidine, may be useful if there are significant symptoms of "over-arousal". These may inhibit the formation of traumatic memories by blocking adrenaline's effects on the amygdala.[110]
Glucocorticoids. There is some evidence suggesting that administering glucocorticoids immediately after a traumatic experience may help prevent PTSD. Several studies have shown that individuals who receive high doses of hydrocortisone for treatment of septic shock, or following surgery, have a lower incidence and fewer symptoms of PTSD.[111][112][113]
Psychobiological treatments have also found success, especially with cortisol.[97] Psychobiological treatments target biological changes that occur after a traumatic event. They also attempt to chemically alter learning or memory formation. Cortisol treatments after a traumatic event have found success in mitigating later diagnosis of PTSD. As discussed earlier, cortisol is often lower in individuals who are at risk of PTSD after a traumatic event than their counterparts. By increasing cortisol levels to normal levels this has been shown to reduce arousal post event as well prevent GR upregulation.
Management[]
Psychological[]
Many forms of psychotherapy have been advocated for trauma-related problems such as PTSD. Basic counseling practices common to many treatment responses for PTSD include education about the condition and provision of safety and support.[49][114]
The psychotherapy programs with the strongest demonstrated efficacy include cognitive behavioral programs, variants of exposure therapy, stress inoculation training (SIT), variants of cognitive therapy (CT), eye movement desensitization and reprocessing (EMDR),[75] and many combinations of these procedures.[115][116] A 2010 review disagrees that these treatments have proven efficacy and points out methodological flaws in the studies and previous meta-analyses.[117]
EMDR and trauma-focused cognitive behavioral therapy (TFCBT) were recommended as first-line treatments for trauma victims in a 2007 review; however, "the evidence base [for EMDR] was not as strong as that for TFCBT ... Furthermore, there was limited evidence that TFCBT and EMDR were superior to supportive/non-directive treatments, hence it is highly unlikely that their effectiveness is due to non-specific factors such as attention."[118] A meta-analytic comparison of EMDR and cognitive behavioral therapy found both protocols indistinguishable in terms of effectiveness in treating PTSD; however, "the contribution of the eye movement component in EMDR to treatment outcome" is unclear.[119]
Cognitive behavioral therapy[]
Cognitive behavioral therapy (CBT) seeks to change the way a trauma victim feels and acts by changing the patterns of thinking or behavior, or both, responsible for negative emotions. CBT has been proven to be an effective treatment for PTSD and is currently considered the standard of care for PTSD by the United States Department of Defense.[120] In CBT, individuals learn to identify thoughts that make them feel afraid or upset and replace them with less distressing thoughts. The goal is to understand how certain thoughts about events cause PTSD-related stress.
Recent research on contextually based third-generation behavior therapies suggests that they may produce results comparable to some of the better validated therapies.[121] Many of these therapy methods have a significant element of exposure[122] and have demonstrated success in treating the primary problems of PTSD and co-occurring depressive symptoms.[123]
Exposure therapy is a type of cognitive behavioral therapy[124] that involves assisting trauma survivors to re-experience distressing trauma-related memories and reminders in order to facilitate habituation and successful emotional processing of the trauma memory. Most exposure therapy programs include both imaginal confrontation with the traumatic memories and real-life exposure to trauma reminders; this therapy modality is well supported by clinical evidence. The success of exposure-based therapies has raised the question of whether exposure is a necessary ingredient in the treatment of PTSD.[125] Some organizations[which?] have endorsed the need for exposure.[126][127] The US Department of Veterans Affairs has been actively training mental health treatment staff in prolonged exposure therapy[128] and Cognitive Processing Therapy[129] in an effort to better treat US Veterans with PTSD.
Eye movement desensitization and reprocessing[]
Eye movement desensitization and reprocessing (EMDR) is a form of psychotherapy developed and studied by Francine Shapiro.[130] She had noticed that when she was thinking about disturbing memories herself, her eyes were moving rapidly. When she brought her eye movements under control while thinking, the thoughts were less distressing.[130]
In 2002, Shapiro and Maxfield published a theory of why this might work, called adaptive information processing.[131] This theory proposes that eye movement can be used to facilitate emotional processing of memories, changing the person's memory to attend to more adaptive information.[132] The therapist initiates voluntary rapid eye movements while the person focuses on memories, feelings or thoughts about a particular trauma.[2][133] The therapists uses hand movements to get the person to move their eyes backwards and forwards, but hand-tapping or tones can also be used.[2] EMDR closely resembles cognitive behavior therapy as it combines exposure (re-visiting the traumatic event), working on cognitive processes and relaxation/self-monitoring.[2] However, exposure by way of being asked to think about the experience rather than talk about it has been highlighted as one of the more important distinguishing elements of EMDR.[134]
There have been multiple small controlled trials of four to eight weeks of EMDR in adults[135] as well as children and adolescents.[133] EMDR reduced PTSD symptoms enough in the short term that one in two adults no longer met the criteria for PTSD, but the number of people involved in these trials was small.[135] There was not enough evidence to know whether or not EMDR could eliminate PTSD.[135] There was some evidence that EMDR might prevent depression.[135] There were no studies comparing EMDR to other psychological treatments or to medication.[135] Adverse effects were largely unstudied.[135] The benefits were greater for women with a history of sexual assault compared with people who had experienced other types of traumatizing events (such as accidents, physical assaults and war). There is a small amount of evidence that EMDR may improve re-experiencing symptoms in children and adolescents, but EMDR has not been shown to improve other PTSD symptoms, anxiety or depression.[133]
The eye movement component of the therapy may not be critical for benefit.[2][132] As there has been no major, high quality randomized trial of EMDR with eye movements versus EMDR without eye movements, the controversy over effectiveness is likely to continue.[134]
Interpersonal psychotherapy[]
Other approaches, particularly involving social supports,[46][47] may also be important. An open trial of interpersonal psychotherapy[136] reported high rates of remission from PTSD symptoms without using exposure.[137] A current, NIMH-funded trial in New York City is now (and into 2013) comparing interpersonal psychotherapy, prolonged exposure therapy, and relaxation therapy.[138][139][140]
Medication[]
A variety of medications has shown adjunctive benefit in reducing PTSD symptoms,[141] but "there is no clear drug treatment for PTSD".[142] Positive symptoms (re-experiencing, hypervigilance, increased arousal) generally respond better to medication than negative symptoms (avoidance, withdrawal), and it is recommended that any drug trial last for at least 6–8 weeks.[142] With many medications, residual symptoms following treatment is the rule rather than the exception, which has led to increased research in the aggressive treatment of PTSD symptoms.[143]
Some studies have shown that treatment with hydrocortisone shortly after a traumatic event, in comparison to a placebo, decreases the likelihood that the patient will suffer from PTSD. Other studies have indicated that propranolol administered within 6 hours of a traumatic event decreases the physiological reactivity to a reminder of the traumatic event. However propranolol had no effect on the rate of PTSD. Despite these studies there is not significant evidence that medication can prevent PTSD, therefore none is routinely administered.[144]
Symptom management[]
SSRIs (selective serotonin reuptake inhibitors). SSRIs are considered to be a first-line drug treatment.[145][146] SSRIs for which there are data to support use include: citalopram, escitalopram,[147] fluoxetine,[148] fluvoxamine,[149] paroxetine,[150] and sertraline.[148][151]
Among the anti-depressants described in this section, bupropion and venlafaxine have the lowest patient drop-out rates. Sertraline, fluoxetine, and nefazodone have a modestly higher drop-out rate (~15%), and the heterocyclics and paroxetine have the highest rates (~20%+).[152] Where drop-out is caused or feared because of medication side-effects, it should be remembered that most patients do not experience such side-effects.[153]
Tricyclic antidepressants. Amitriptyline ("Elavil") has shown benefit for positive distress symptoms and for avoidance, and imipramine ("Tofranil") has shown benefit for intrusive symptoms.[148]
Alpha-adrenergic antagonists. Prazosin ("Minipress"), in a small study of combat veterans, has shown substantial benefit in relieving or reducing nightmares.[50] Clonidine ("Catapres") can be helpful with startle, hyperarousal, and general autonomic hyperexcitability.[154]
Anti-convulsants, mood stabilizers, anti-aggression agents. Carbamazepine ("Tegretol") has likely benefit in reducing arousal symptoms involving noxious affect,[148] as well as mood or aggression.[155] Topiramate ("Topamax")[50] has been effective in achieving major reductions in flashbacks and nightmares, and no reduction of effect was seen over time.[50] Zolpidem ("Ambien") has also proven useful in treating sleep disturbances.[154]
Lamotrigine ("Lamictal") may be useful in reducing reexperiencing symptoms, as well as avoidance and emotional numbing.[50][156][157][158] Valproic acid ("Depakene") and has shown reduction of symptoms of irritability, aggression, and impulsiveness, and in reducing flashbacks.[154] Similarly, lithium carbonate has worked to control mood and aggressions (but not anxiety) symptoms.[155] Buspirone ("BuSpar") has an effect similar to that of lithium, with the additional benefit of working to reduce hyperarousal symptoms.[154]
Antipsychotics. Risperidone can be used to help with dissociation, mood issues, and aggression.[159]
Serotonin antagonists. Cyproheptadine (Periactin) can be used to help with sleep disorders and nightmares.[160]
Atypical antidepressants.[161] Nefazodone ("Serzone") can be effective with sleep disturbance symptoms and with secondary depression, anxiety, and sexual dysfunction symptoms.[148] Trazodone ("Desyrel") can also reduce or eliminate problems with anger, anxiety, and disturbed sleep.[148]
Beta blockers. Propranolol ("Inderal") has demonstrated possibilities in reducing hyperarousal symptoms, including sleep disturbances.[110][154]
Benzodiazepines. These drugs are not recommended by clinical guidelines for the treatment of PTSD due to a lack of evidence of benefit.[162] Nevertheless some doctors use benzodiazepines with caution for short-term anxiety relief,[159][163] hyperarousal, and sleep disturbance.[154] However, some authors believe that the use of benzodiazepines is contraindicated for acute stress as this group of drugs promote dissociation and ulterior revivals.[164] While benzodiazepines can alleviate acute anxiety, there is no consistent evidence that they can stop the development of PTSD, or are at all effective in the treatment of posttraumatic stress disorder. Additionally, benzodiazepines may reduce the effectiveness of psychotherapeutic interventions, and there is some evidence that benzodiazepines may actually contribute to the development and chronification of PTSD. Other drawbacks include the risk of developing a benzodiazepine dependence and withdrawal syndrome; additionally, individuals with PTSD are at an increased risk of abusing benzodiazepines.[145][165]
Glucocorticoids. Additionally, post-stress high dose corticosterone administration was recently found to reduce "PTSD-like" behaviors in a rat model of PTSD. In this study, corticosterone impaired memory performance, suggesting that it may reduce risk for PTSD by interfering with consolidation of traumatic memories.[166] The neurodegenerative effects of the glucocorticoids, however, may prove this treatment counterproductive.[167]
Monoamine-oxidase inhibitors (MAOIs). Phenelzine ("Nardil") has for some time[when?] been observed to be effective with hyperarousal and depression and is especially effective with nightmares.[148]
Miscellaneous other medications. Clinical trials evaluating methylenedioxymethamphetamine (MDMA, "Ecstasy") in conjunction with psychotherapy are being conducted in Switzerland[168] and Israel.[169]
Medications by symptom group affected[]
Medications can affect one or more of the symptoms, in one or more of the three major symptom classes[3] involved in diagnosing PTSD, which can be summarized in the following table:[159][163][170]
| Symptom class | Symptom | Medication |
|---|---|---|
| Reexperiencing | ||
| intrusive recall | amitriptyline; fluoxetine; imipramine; lamotrigine; sertraline | |
| intrusive reexperiencing | amitriptyline; fluoxetine; imipramine; nefazodone; sertraline (women only); topiramate; | |
| sleep disturbance, nightmares | benzodiazepines; carbamazepine; clonidine; nefazodone; phenelzine; prazosin; topiramate; trazodone; zolpidem | |
| dissociative recall | risperidone | |
| intense psychological distress (anger, anxiety) when exposed to reminders of traumatic event(s) | benzodiazepines; buspirone; carbamazepine; lithium (not for anxiety); nefazodone; trazodone | |
| Avoidance | ||
| avoidance | amitriptyline; fluoxetine; lamotrigine; nefazodone; sertraline | |
| feelings of detachment or estrangement from others | amitriptyline; risperidone | |
| restricted range of affect (numbing) | amitriptyline; lamotrigine; sertraline (women only) | |
| Hyperarousal | ||
| general hyperarousal | amitriptyline; nefazodone; phenelzine; sertraline (women only) | |
| sleep disturbance, nightmares | benzodiazepines; carbamazepine; clonidine; nefazodone; phenelzine; trazodone; zolpidem | |
| irritability, anger (and impulsiveness) | carbamazepine; nefazodone; valproic acid | |
| anger | buspirone; fluoxetine; lithium; trazodone | |
| aggression | risperidone | |
| exaggerated startle response; general autonomic hyperexcitability | benzodiazepines; buspirone; carbamazepine; clonidine; propranolol; valproic acid | |
Some medications can also help with symptoms which may occur secondary to PTSD:[170]
| Secondary symptom | Medication |
|---|---|
| depression | nefazodone; phenelzine |
| dream content distortions | nefazodone |
| relapse of symptoms | carbamazepine |
| self-mutilation | clonidine; buprenorphine |
| sexual function reduction | nefazodone |
| sleep hours reduction | nefazodone |
Other[]
- Exercise, sport and physical activity
Physical activity can have an impact on people's psychological wellbeing[171] and physical health.[172] The U.S. National Center for PTSD recommends moderate exercise as a way to distract from disturbing emotions, build self-esteem and increase feelings of being in control again. They recommend a discussion with a doctor before starting an exercise program.[173]
Some uncontrolled studies have found benefits for people with PTSD from exercise programs.[171] A small trial studied adding a physical component to biofeedback-based CBT with traumatized refugees. The authors concluded that physical activity may lead to clinical improvement, but bigger trials are needed.[174] More trials are underway.[175][176][177]
- Play therapy for children
Play is thought to help children link their inner thoughts with their outer world, connecting real experiences with abstract thought.[178] Repetitive play can also be one of the ways a child relives traumatic events, and that can be a symptom of traumatization in a child or young person.[179]
Play is a familiar way for children and young people to indirectly address what worries them, so it is often used as an element of psychological treatment - for example using play materials or drawing to help a child focus on their feelings and events.[2][178] Play therapy means using games, drawings and play materials to express, understand and control feelings rather than as a means of communication.[178][180] Although it is commonly used, there have not been enough studies comparing outcomes in groups of children receiving and not receiving play therapy, so the effects of play therapy are not yet understood.[2][178]
Epidemiology[]


{kind=link}
Disability-adjusted life year rates for posttraumatic stress disorder per 100,000 inhabitants in 2004.[181]
There is debate over the rates of PTSD found in populations, but despite changes in diagnosis and the criteria used to define PTSD between 1997 and 2007, epidemiological rates have not changed significantly.[182]
The United Nations' World Health Organization publishes estimates of PTSD impact for each of its member states; the latest data available are for 2004. Considering only the 25 most populated countries,[183] ranked by overall age-standardized Disability-Adjusted Life Year (DALY) rate, the top half of the ranked list is dominated by Asian/Pacific countries, the USA, and Egypt.[184] Ranking the countries by the male-only or female-only rates produces much the same result, but with less meaningfulness, as the score range in the single sex rankings is much reduced (4 for women, 3 for men, as compared with 14 for the overall score range), suggesting that the differences between female and male rates, within each country, is what drives the distinctions between the countries.[185][186]
| Region | Country | PTSD DALY rate, overall |
[184] PTSD DALY rate, females |
[185] PTSD DALY rate, males[186] |
|---|---|---|---|---|
| Asia / Pacific | Thailand | 59 | 86 | 30 |
| Asia / Pacific | Indonesia | 58 | 86 | 30 |
| Asia / Pacific | Philippines | 58 | 86 | 30 |
| Americas | USA | 58 | 86 | 30 |
| Asia / Pacific | Bangladesh | 57 | 85 | 29 |
| Africa | Egypt | 56 | 83 | 30 |
| Asia / Pacific | India | 56 | 85 | 29 |
| Asia / Pacific | Iran | 56 | 83 | 30 |
| Asia / Pacific | Pakistan | 56 | 85 | 29 |
| Asia / Pacific | Japan | 55 | 80 | 31 |
| Asia / Pacific | Myanmar | 55 | 81 | 30 |
| Europe | Turkey | 55 | 81 | 30 |
| Asia / Pacific | Vietnam | 55 | 80 | 30 |
| Europe | France | 54 | 80 | 28 |
| Europe | Germany | 54 | 80 | 28 |
| Europe | Italy | 54 | 80 | 28 |
| Asia / Pacific | Russian Federation | 54 | 78 | 30 |
| Europe | United Kingdom | 54 | 80 | 28 |
| Africa | Nigeria | 53 | 76 | 29 |
| Africa | Dem. Republ. of Congo | 52 | 76 | 28 |
| Africa | Ethiopia | 52 | 76 | 28 |
| Africa | South Africa | 52 | 76 | 28 |
| Asia / Pacific | China | 51 | 76 | 28 |
| America | Mexico | 46 | 60 | 30 |
| America | Brazil | 45 | 60 | 30 |
United States[]
The National Comorbidity Survey Replication has estimated that the lifetime prevalence of PTSD among adult Americans is 6.8%, with women (9.7%) more than twice as likely as men[18] (3.6%) to have PTSD at some point in their lives.[187] More than 60% of men and more than 60% of women experience at least one traumatic event in their life. The most frequently reported traumatic events by men are rape, combat, and childhood neglect or physical abuse. Women most frequently report instances of rape, sexual molestation, physical attack, being threatened with a weapon and childhood physical abuse.[18] 88% of men and 79% of women with lifetime PTSD have at least one comorbid psychiatric disorder. Major depressive disorder, 48% of men and 49% of women, and lifetime alcohol abuse or dependence, 51.9% of men and 27.9% of women, are the most common comorbid disorders.[188]
The United States Department of Veterans Affairs estimates that 830,000 Vietnam War veterans suffered symptoms of PTSD.[189] The National Vietnam Veterans' Readjustment Study (NVVRS) found 15.2% of male and 8.5% of female Vietnam Vets to suffer from current PTSD at the time of the study. Life-Time prevalence of PTSD was 30.9% for males and 26.9% for females. In a reanalysis of the NVVRS data, along with analysis of the data from the Matsunaga Vietnam Veterans Project, Schnurr, Lunney, Sengupta, and Waelde found that, contrary to the initial analysis of the NVVRS data, a large majority of Vietnam veterans suffered from PTSD symptoms (but not the disorder itself). Four out of five reported recent symptoms when interviewed 20–25 years after Vietnam.[45]
A 2011 study from Georgia State University and San Diego State University found that rates of PTSD diagnosis increased significantly when troops were stationed in combat zones, had tours of longer than a year, experienced combat, or were injured. Military personnel serving in combat zones were 12.1 percentage points more likely to receive a PTSD diagnosis than their active-duty counterparts in non-combat zones. Those serving more than 12 months in a combat zone were 14.3 percentage points more likely to be diagnosed with PTSD than those who served less than one year. Experiencing an enemy firefight was associated a 18.3 percentage point increase in the probability of PTSD, while being wounded or injured in combat was associated a 23.9 percentage point increase in the likelihood of a PTSD diagnosis. For the 2.16 million U.S. troops deployed in combat zones between 2001 and 2010, the total estimated two-year costs of treatment for combat-related PTSD are between $1.54 billion and $2.69 billion.[190]
Society and culture[]


{kind=link}
United States—veterans[]
A review of the provision of compensation to veterans for PTSD by the United States Department of Veterans Affairs began in 2005 after the VA had noted a 30% increase in PTSD claims in recent years.[191] In 2005 the suicide rate among male Veteran VA users was 37.19 per 100,000, compared to 13.59 in females.[192] This led to a backlash from veterans'-rights groups, and to some highly publicized suicides by veterans who feared losing their benefits,[citation needed] which in some cases constituted their only income. In response, on November 10, 2005, the Secretary of Veterans Affairs announced that "the Department of Veterans Affairs (VA) will not review the files of 72,000 veterans currently receiving disability compensation for posttraumatic stress disorder..."[193]
Many veterans of the wars in Iraq and Afghanistan have faced significant physical, emotional, and relational disruptions. In response, the United States Marine Corps has instituted programs to assist them in re-adjusting to civilian life, especially in their relationships with spouses and loved ones, to help them communicate better and understand what the other has gone through.[194] Walter Reed Army Institute of Research (WRAIR) developed the Battlemind program to assist service members avoid or ameliorate PTSD and related problems.
The American Legion is the most popular social and mutual-aid veterans' organization, with nearly 3 million members in over 14,000 Posts. Posts organize community events and service projects, and often have a bar open for limited hours. The American Legion is politically active on behalf of interests of veterans and service members, promoting support for veterans benefits, Veterans Affairs hospital system.[195]
The Sierra Club Military Families and Veterans Initiative organizes wilderness trips for veterans, and has received positive feedback about stress reduction.[196] One viewpoint suggests that "the key seems to be helping vets experience intense challenges free from the psychological shackles of life-and-death danger." Ice climbing has been a successful activity, "because its perceived challenge is so high,"[197] and Grizzly Tracking in Montana for Veterans, Service Members, and Families is scheduled for summer 2012.[198] More relaxing wilderness trips may also be of value, as settling into a rhythm moves an individual away from a state of hypervigilance into a more relaxed "flow experience". A Colorado therapist has suggested that "repetitive motor movements like cycling or skiing" and "rhythmic outdoor activities" reduce stress through a mechanism similar to EMDR therapy. An Outward Bound instructor comments that "the most healing occurs while [people are] drinking coffee and hanging out by the river" with fellow vets.[197]
Other countries—veterans[]
In the UK, there has been some controversy that National Health Service is dumping veterans on service charities like Combat Stress.[199][200][201]
Veterans Affairs Canada offers a new program that includes rehabilitation, financial benefits, job placement, health benefits program, disability awards, peer support[202][203][204] and family support.[205]
History[]
Earliest reports[]
Psychiatrist Jonathan Shay has proposed that Lady Percy's soliloquy in Henry IV, Part 1 (act 2,scene 3, lines 40-62), written around 1597, represents an unusually accurate description of the symptom constellation of PTSD.[206]
Military settings[]


{kind=link}
Statue, Three Servicemen, Vietnam Veterans Memorial
According to Stéphane Audoin-Rouzeau and Annette Becker, "One-tenth of mobilized American men were hospitalized for mental disturbances between 1942 and 1945, and after thirty-five days of uninterrupted combat, 98% of them manifested psychiatric disturbances in varying degrees."[207]
Although PTSD-like symptoms have also been recognized in combat veterans of many military conflicts since, the modern understanding of PTSD dates from the 1970s, largely as a result of the problems that were still being experienced by US military veterans of the war in Vietnam.[208]
Previous diagnoses now considered historical equivalents of PTSD include railway spine, stress syndrome, shell shock, battle fatigue, or traumatic war neurosis.[209]
Terminology[]
The term post-traumatic stress disorder (PTSD) was coined in the mid 1970s,[208] in part through the efforts of anti–Vietnam War activists and the anti-war group Vietnam Veterans Against the War and Chaim F. Shatan, who worked with them and coined the term post-Vietnam Syndrome; the condition was added to the DSM-III as posttraumatic stress disorder.[210]
Early in 1978, the term was used in a working group finding presented to the Committee of Reactive Disorders.[210] The term was formally recognized in 1980.[208]
In the DSM-IV, the spelling "posttraumatic stress disorder" is used, while in the ICD-10 the spelling is "post-traumatic stress disorder".[211] Elsewhere, especially in less formal writing, the term may be rendered as two words—"post traumatic stress disorder".[citation needed])
See also[]
Notes[]
- ↑ Acceptable variants of this term exist; see Terminology section in this article.
References[]
- ↑ 1.0 1.1 1.2 American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (Fifth ed.). Arlington, VA: American Psychiatric Publishing. pp. 271–280. ISBN 978-0-89042-555-8.
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 2.12 2.13 2.14 National Collaborating Centre for Mental Health (UK) (2005). "Post-Traumatic Stress Disorder: The Management of PTSD in Adults and Children in Primary and Secondary Care". NICE Clinical Guidelines, No. 26. Gaskell (Royal College of Psychiatrists). http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0015848/. Retrieved 1 June 2013.
- ↑ 3.0 3.1 3.2 3.3 3.4 3.5 American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders: DSM-IV. Washington, DC: American Psychiatric Association. ISBN 0-89042-061-0.; on-line.
- ↑ Rothschild, Babette (200). The Body Remembers: The Psychophysiology of Trauma and Trauma Treatment. New York: W.W. Norton & Company. ISBN 0393703274.
- ↑ Kaplan, HI; Sadock, BJ, Grebb, JA (1994). Kaplan and Sadock's synopsis of psychiatry: Behavioral sciences, clinical psychiatry, 7th ed.. Baltimore: Williams & Williams. pp. 606–609.
- ↑ Satcher D et al. (1999). "Chapter 4". Mental Health: A Report of the Surgeon General. Surgeon General of the United States. http://www.surgeongeneral.gov/library/mentalhealth/toc.html#chapter4.
- ↑ Robinson, Maisah (May 27, 2006). "Review of Francisco Goya's Disasters of War". Associated Press. http://voices.yahoo.com/review-francisco-goyas-disasters-war-40022.html.
- ↑ "Post-Traumatic Stress Disorder (PTSD)". National Institute of Mental Health (NIMH), U.S. Department of Health and Human Services. http://www.nimh.nih.gov/health/publications/post-traumatic-stress-disorder-ptsd/who-gets-ptsd.shtml. Retrieved 2011-12-16.
- ↑ Mayo Clinic staff. "Post-traumatic stress disorder (PTSD)". Mayo Foundation for Medical Education and Research. http://www.mayoclinic.com/health/post-traumatic-stress-disorder/DS00246/DSECTION=causes. Retrieved 2011-12-16.
- ↑ 10.0 10.1 Fullerton, CS; Ursano, Wang (2004). "Acute Stress Disorder, Posttraumatic Stress Disorder, and Depression in Disaster or Rescue Workers". pp. 1370–1376. Digital object identifier:10.1176/appi.ajp.161.8.1370. PMID 15285961.
- ↑ Kelleher I, Harley M, Lynch F, Arseneault L, Fitzpatrick C, Cannon M (November 2008). "Associations between childhood trauma, bullying and psychotic symptoms among a school-based adolescent sample". pp. 378–82. Digital object identifier:10.1192/bjp.bp.108.049536. PMID 18978317.
- ↑ "Are they really out to get your patient?" http://web.archive.org/web/20100509035009/http://www.innovations-training.com/0804CP_Article4.pdf Current Psychiatry Volume 8 Number 4
- ↑ McCloskey, Laura Ann; Marla Walker (January 2000). "Posttraumatic Stress in Children Exposed to Family Violence and Single-Event Trauma". pp. 108–115. Digital object identifier:10.1097/00004583-200001000-00023. http://www.sciencedirect.com/science/article/pii/S0890856709661074.
- ↑ Binder EB, Bradley RG, Liu W, et al. (March 2008). "Association of FKBP5 polymorphisms and childhood abuse with risk of posttraumatic stress disorder symptoms in adults". pp. 1291–305. Digital object identifier:10.1001/jama.299.11.1291. PMC 2441757. PMID 18349090.
- ↑ Peggy Peck, Executive Editor (2008-03-09). "Genes May Affect Lifelong Impact of Child Abuse". MedPage Today. http://www.medpagetoday.com/Genetics/GeneticTesting/dh/8824.
- ↑ Constance Holden (2008-03-18). "Seeds of PTSD Planted in Childhood". ScienceNOW Daily News. http://sciencenow.sciencemag.org/cgi/content/full/2008/318/2?etoc.
- ↑ Rothschild, Babette (2000). The Body Remembers: The psychophysiology of Trauma and Trauma Treatment. New York: W.W. Norton & Company. ISBN 0393703274.
- ↑ 18.0 18.1 18.2 18.3 18.4 18.5 18.6 18.7 18.8 Olszewski, Terese M.; Jeanne F. Varrasse (June 2005). "The Neurobiology of PTSD". pp. 40.
- ↑ Ehlers, A., Hackmann, A., & Michael, T. (2004). Intrusive re-experiencing in post-traumatic stress disorder: Phenomenology, theory, and therapy. Memory, 12(4), 403-415. doi:10.1080/09658210444000025
- ↑ Schechter DS, Coates SW, Kaminer T, et al. (2008). "Distorted maternal mental representations and atypical behavior in a clinical sample of violence-exposed mothers and their toddlers". pp. 123–47. Digital object identifier:10.1080/15299730802045666. PMC 2577290. PMID 18985165.
- ↑ Schechter DS, Zygmunt A, Coates SW, et al. (September 2007). "Caregiver traumatization adversely impacts young children's mental representations on the MacArthur Story Stem Battery". pp. 187–205. Digital object identifier:10.1080/14616730701453762. PMC 2078523. PMID 18007959.
- ↑ Schechter DS, Gross A, Willheim E, et al. (December 2009). "Is maternal PTSD associated with greater exposure of very young children to violent media?". pp. 658–62. Digital object identifier:10.1002/jts.20472. PMC 2798921. PMID 19924819.
- ↑ Clarke, C. et al. 2007. Childhood and Adulthood Psychological Ill Health as Predictors of Midlife and Anxiety disorders. Archives of General Psychiatry. 64. pp668-678
- ↑ Chris Cantor (2005). Evolution and posttraumatic stress: disorders of vigilance and defence. Routledge. ISBN 978-1-58391-771-8. http://books.google.com/books?id=yBavaOGUd_MC&pg=PR3.
- ↑ doi:10.1080/00048670701261178
This citation will be automatically completed in the next few minutes. You can jump the queue or expand by hand - ↑ doi:10.1016/j.pnpbp.2006.01.008
This citation will be automatically completed in the next few minutes. You can jump the queue or expand by hand - ↑ True WR, Rice J, Eisen SA, et al. (1993). "A twin study of genetic and environmental contributions to liability for posttraumatic stress symptoms". pp. 257–64. Digital object identifier:10.1001/archpsyc.1993.01820160019002. PMID 8466386.
- ↑ 28.00 28.01 28.02 28.03 28.04 28.05 28.06 28.07 28.08 28.09 28.10 28.11 28.12 28.13 Skelton, Kelly; Kerry J. Ressler, Seth D. Norrholm, Tanja Jovanovic, Bekh Bradley-Davino (2012). "PTSD and gene variants: New pathways and new thinking". pp. 628–637. Digital object identifier:10.1016/j.neuropharm.2011.02.013. PMC 3136568. PMID 21356219.
- ↑ Newton, Phil (16 November 2008) "A gene for anxiety, depression and posttraumatic stress disorder; FKBP5" Psychology Today. Accessed 29 November 2011.
- ↑ Binder EB, Bradley RG, Liu W, et al. (2008). "Association of FKBP5 polymorphisms and childhood abuse with risk of posttraumatic stress disorder symptoms in adults". pp. 1291–305. Digital object identifier:10.1001/jama.299.11.1291. PMC 2441757. PMID 18349090.
- ↑ Koenen KC, Saxe G, Purcell S, et al. (2005). "Polymorphisms in FKBP5 are associated with peritraumatic dissociation in medically injured children". pp. 1058–9. Digital object identifier:10.1038/sj.mp.4001727. PMID 16088328.
- ↑ Birmes P, Brunet A, Carreras D, et al. (2003). "The predictive power of peritraumatic dissociation and acute stress symptoms for posttraumatic stress symptoms: a three-month prospective study". pp. 1337–9. Digital object identifier:10.1176/appi.ajp.160.7.1337. PMID 12832251.
- ↑ 33.0 33.1 Schnurr PP, Lunney CA, Sengupta A (2004). "Risk factors for the development versus maintenance of posttraumatic stress disorder". pp. 85–95. Digital object identifier:10.1023/B:JOTS.0000022614.21794.f4. PMID 15141781.
- ↑ Yehuda R, Cai G, Golier JA, Sarapas C, Galea S, Ising M, Rein T, Schmeidler J, Müller-Myhsok B, Holsboer F, Buxbaum JD (24 April 2009 [Epub ahead of print]). "Gene expression patterns associated with posttraumatic stress disorder following exposure to the World Trade Center attacks". pp. 708–11. Digital object identifier:10.1016/j.biopsych.2009.02.034. PMID 19393990.
- ↑ Ressler KJ, Merer KB, Bradley B, et al. (February 24, 2011). "Post-traumatic stress disdorder is associated with PACAP and the PAC1 receptor". pp. 492–497. Digital object identifier:10.1038/nature09856. PMC 3046811. PMID 21350482.
- ↑ 36.0 36.1 Spoont, Michele; Arbisi P, Fu S, Greer N, Kehle-Forbes S, Meis L, Rutks I. (January 2013). "Screening for Post-Traumatic Stress Disorder (PTSD) in Primary Care: A Systematic Review". Washington DC: Department of Veterans Affairs. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0053614/. Retrieved 1 June 2013.
- ↑ Koenen KC, Moffitt TE, Poulton R, Martin J, Caspi A (February 2007). "Early childhood factors associated with the development of post-traumatic stress disorder: results from a longitudinal birth cohort". pp. 181–92. Digital object identifier:10.1017/S0033291706009019. PMC 2254221. PMID 17052377.
- ↑ Lapp KG, Bosworth HB, Strauss JL, et al. (September 2005). "Lifetime sexual and physical victimization among male veterans with combat-related post-traumatic stress disorder". pp. 787–90. PMID 16261985.
- ↑ Otte C, Neylan TC, Pole N, et al. (January 2005). "Association between childhood trauma and catecholamine response to psychological stress in police academy recruits". pp. 27–32. Digital object identifier:10.1016/j.biopsych.2004.10.009. PMID 15607297.
- ↑ Resnick HS, Yehuda R, Pitman RK, Foy DW (November 1995). "Effect of previous trauma on acute plasma cortisol level following rape". pp. 1675–7. PMID 7485635. http://ajp.psychiatryonline.org/cgi/pmidlookup?view=long&pmid=7485635.
- ↑ Laor N, Wolmer L, Mayes LC, et al. (May 1996). "Israeli preschoolers under Scud missile attacks. A developmental perspective on risk-modifying factors". pp. 416–23. Digital object identifier:10.1001/archpsyc.1996.01830050052008. PMID 8624185.
- ↑ Laor N, Wolmer L, Mayes LC, Gershon A, Weizman R, Cohen DJ (March 1997). "Israeli preschool children under Scuds: a 30-month follow-up". pp. 349–56. Digital object identifier:10.1097/00004583-199703000-00013. PMID 9055515. http://meta.wkhealth.com/pt/pt-core/template-journal/lwwgateway/media/landingpage.htm?issn=0890-8567&volume=36&issue=3&spage=349.
- ↑ Janoff-Bulman R: Shattered Assumptions: Toward a New Psychology of Trauma. New York: Free Press, 1992.
- ↑ Falsetti, Sherry A.; Monier, Jeannine; Resnick, Jeannine (2005). "Chapter 2: Intrusive Thoughts In Posttraumatic Stress Disorder". In Clark, David A.. Intrusive Thoughts In Clinical Disorders. Theory, Research, and Treatment. The Guilford Press. pp. 40–41. ISBN 1-59385-083-2.
- ↑ 45.0 45.1 Jennifer L. Price, Ph.D.: Findings from the National Vietnam Veterans' Readjustment Study - Factsheet. National Center for PTSD. United States Department of Veterans Affairs [1].
- ↑ 46.0 46.1 Brewin CR, Andrews B, Valentine JD (October 2000). "Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults". pp. 748–66. Digital object identifier:10.1037/0022-006X.68.5.748. PMID 11068961. http://content.apa.org/journals/ccp/68/5/748.
- ↑ 47.0 47.1 Ozer EJ, Best SR, Lipsey TL, Weiss DS (January 2003). "Predictors of posttraumatic stress disorder and symptoms in adults: a meta-analysis". pp. 52–73. Digital object identifier:10.1037/0033-2909.129.1.52. PMID 12555794. http://content.apa.org/journals/bul/129/1/52.
- ↑ Psychiatry In The U.S. Army: Lessons for Community Psychiatry By Albert Julius Glass, Franklin D. Jones [2]
- ↑ 49.0 49.1 49.2 Rothschild, Babette (2000). The Body Remembers: The Psychophysiology of Trauma and Trauma Treatment. New York: W.W. Norton & Company. ISBN 0393703274.
- ↑ 50.0 50.1 50.2 50.3 50.4 50.5 Maxmen, J. S.; Ward, N. G. (2002). Psychotropic drugs: fast facts (third ed.). New York: W. W. Norton. p. 348. ISBN 0-393-70301-0.
- ↑ Cohen SI (February 1995). "Alcohol and benzodiazepines generate anxiety, panic and phobias". pp. 73–77. PMC 1295099. PMID 7769598.
- ↑ Spates, R. & Souza (2007). Treatment of PTSD and Substance Abuse Comorbidity. The Behavior Analyst Today 9 (1 11-26 [3]
- ↑ "Former Foster Children in Oregon and Washington Suffer Posttraumatic Stress Disorder at Twice the Rate of U.S War Veterans". Casey Family Programs, Harvard Medical School. 2005.04.05. Archived from the original on 2005-05-11. http://web.archive.org/web/20050511053720/http://www.jimcaseyyouth.org/docs/nwa_release.pdf. Retrieved 2010-03-23.
- ↑ Casey Family Programs (2005). "Assessing the Effects of Foster Care: Mental Health Outcomes from the Casey National Alumni Study". http://www.casey.org/Resources/Publications/pdf/CaseyNationalAlumniStudy_MentalHealth.pdf.
- ↑ Dubner AE, Motta RW (June 1999). "Sexually and physically abused foster care children and posttraumatic stress disorder". pp. 367–73. Digital object identifier:10.1037/0022-006X.67.3.367. PMID 10369057.
- ↑ PBS Series "The Secret Life of the Brain Episode 4, 2001
- ↑ Zohar, Joseph; Alzbeta Juven-Wetzler, Viki Myers, and Leah Fostic (2008). "Post-Traumatic stress disorder: Facts and Fiction". pp. 70–eoa. Digital object identifier:10.1097/YCO.0b013e3282f269ee.
- ↑ Yehuda R, Halligan SL, Golier JA, Grossman R, Bierer LM (2004). "Effects of trauma exposure on the cortisol response to dexamethasone administration in PTSD and major depressive disorder". pp. 389–404. Digital object identifier:10.1016/S0306-4530(03)00052-0. PMID 14644068.
- ↑ Yehuda R, Halligan SL, Grossman R, Golier JA, Wong C (2002). "The cortisol and glucocorticoid receptor response to low dose dexamethasone administration in aging combat veterans and holocaust survivors with and without posttraumatic stress disorder". pp. 393–403. Digital object identifier:10.1016/S0006-3223(02)01357-4. PMID 12242055.
- ↑ Heim, Christine; Ulrike Ehlert, Dirk H. Hellhammer (2000). "The potential role of hypocorticolism in the pathophysiology of stress-related bodily disorders". pp. 1–35. Digital object identifier:10.1016/S0306-4530(99)00035-9.
- ↑ Mason JW, Giller EL, Kosten TR, Harkness L (1988). "Elevation of urinary norepinephrine/cortisol ratio in posttraumatic stress disorder". pp. 498–502. Digital object identifier:10.1097/00005053-198808000-00008. PMID 3404142.
- ↑ Bohnen N, Nicolson N, Sulon J, Jolles J (1991). "Coping style, trait anxiety and cortisol reactivity during mental stress". pp. 141–7. Digital object identifier:10.1016/0022-3999(91)90068-Y. PMID 2046048.
- ↑ Geracioti TD Jr, Baker DG, Ekhator NN, West SA, Hill KK, Bruce AB, Schmidt D, Rounds-Kugler B, Yehuda R, Keck PE Jr, Kasckow JW (2001). "CSF norepinephrine concentrations in posttraumatic stress disorder". pp. 1227–1230. Digital object identifier:10.1176/appi.ajp.158.8.1227. PMID 11481155.
- ↑ Sautter FJ, Bissette G, Wiley J, et al. (December 2003). "Corticotropin-releasing factor in posttraumatic stress disorder (PTSD) with secondary psychotic symptoms, nonpsychotic PTSD, and healthy control subjects". pp. 1382–8. Digital object identifier:10.1016/S0006-3223(03)00571-7. PMID 14675802.
- ↑ de Kloet CS, Vermetten E, Geuze E, et al. (2008). "Elevated plasma corticotrophin-releasing hormone levels in veterans with posttraumatic stress disorder". pp. 287–91. Digital object identifier:10.1016/S0079-6123(07)67025-3. ISBN 9780444531407. PMID 18037027.
- ↑ Yehuda R (2001). "Biology of posttraumatic stress disorder". pp. 41–6. PMID 11495096.
- ↑ Yehuda R (2002). "Clinical relevance of biologic findings in PTSD". pp. 123–33. Digital object identifier:10.1023/A:1015055711424. PMID 12025720.
- ↑ Aardal-Eriksson E, Eriksson TE, Thorell LH (2001). "Salivary cortisol, posttraumatic stress symptoms, and general health in the acute phase and during 9-month follow-up". pp. 986–93. Digital object identifier:10.1016/S0006-3223(01)01253-7. PMID 11750895.
- ↑ Lindley SE, Carlson EB, Benoit M (2004). "Basal and dexamethasone suppressed salivary cortisol concentrations in a community sample of patients with posttraumatic stress disorder". pp. 940–5. Digital object identifier:10.1016/j.biopsych.2003.12.021. PMID 15110738.
- ↑ "NIMH · Post Traumatic Stress Disorder Research Fact Sheet". National Institutes of Health. http://www.nimh.nih.gov/health/publications/post-traumatic-stress-disorder-research-fact-sheet/index.shtml.
- ↑ [|Newton, Philip]. "From Mouse to Man; the Anatomy of Posttraumatic Stress Disorder". http://www.psychologytoday.com/blog/mouse-man/200901/the-anatomy-post-traumatic-stress-disorder. Retrieved 20 December 2009.
- ↑ Carlson, Neil R. (2007). Physiology of Behavior (9 ed.). Pearson Education, Inc.
- ↑ Jatzko A, Rothenhöfer S, Schmitt A, Gaser C, Demiracka T, Weber-Fahr W, Wessa M, Magnotta V, Braus DF. et al. (2006). "Hippocampal volume in chronic posttraumatic stress disorder (PTSD): MRI study using two different evaluation methods". pp. 121–126. Digital object identifier:10.1016/j.jad.2006.03.010. PMID 16701903.
- ↑ http://dbm.neuro.uni-jena.de/pdf-files/Jatzko-JAD06.pdf
- ↑ 75.0 75.1 Newport, D Jeffery; Charles B Nemeroff (2010). "Neurobiology of posttraumatic stress disorder". pp. 211–218. Digital object identifier:10.1016/S0959-4388(00)00080-5. PMID 10753802.
- ↑ 76.0 76.1 Milad MR, Pitman RK, Ellis CB, Gold AL, Shin LM, Lasko NB, Zeidan MA, Handwerger K, Orr SP et al. (2009). "Neurobiological basis of failure to recall extinction memory in posttraumatic stress disorder". pp. 1075–82. Digital object identifier:10.1016/j.biopsych.2009.06.026. PMC 2787650. PMID 19748076.
- ↑ Stein MB, Paulus MP (2009). "Imbalance of approach and avoidance: the yin and yang of anxiety disorders". pp. 1072–4. Digital object identifier:10.1016/j.biopsych.2009.09.023. PMC 2825567. PMID 19944792.
- ↑ Agis-Balboa RC, Arcos-Diaz D, Wittnam J, Govindarajan N, Blom K, Burkhardt S, Haladyniak U, Agbemenyah HY, Zovoilis A, Salinas-Riester G, Opitz L, Sananbenesi F, Fischer A (August 2011). "A hippocampal insulin-growth factor 2 pathway regulates the extinction of fear memories". pp. 4071–83. Digital object identifier:10.1038/emboj.2011.293. PMC 3209781. PMID 21873981.
- ↑ 79.0 79.1 Radley, Jason J.; Mohamed Kabbaj, Lauren Jacobson, Willem Heydendael, Rachel Yehuda, James P. Harman (September 2011). "Stress risk factors and stress related pathology: Neuroplasticity epigenetics and endophenotypes". pp. 481–497. Digital object identifier:10.3109/10253890.2011.604751. PMC 3641164. PMID 21848436.
- ↑ Pitman RK. (1989). "Post-traumatic stress disorder, hormones, and memory". pp. 221–223. Digital object identifier:10.1016/0006-3223(89)90033-4. PMID 2545287.
- ↑ Zohar, Joseph; Alzbeta Juven-Wetzler, Vicki Myers and Leah Fostic (2008). "Post traumatic stress disorder:facts and fiction". pp. 74–eoa. Digital object identifier:10.1097/YCO.0b013e3282f269ee.
- ↑ "NIMH · What are the symptoms of PTSD?". National Institute of Mental Health. http://www.nimh.nih.gov/health/publications/post-traumatic-stress-disorder-ptsd/what-are-the-symptoms-of-ptsd.shtml.
- ↑ American Psychiatric Association (1987). Diagnostic and Statistical Manual of Mental Disorders: DSM-III-R. ISBN 0-89042-018-1.
- ↑ American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders, quick reference. Washington, D.C.: American Psychiatric Association. p. 211. ISBN 0-89042-063-7.
- ↑ Breslau N, Kessler RC (2001). "The stressor criterion in DSM-IV posttraumatic stress disorder: an empirical investigation". pp. 699–704. Digital object identifier:10.1016/S0006-3223(01)01167-2. PMID 11704077.
- ↑ Blake DD, Weathers FW, Nagy LM, et al. (January 1995). "The development of a Clinician-Administered PTSD Scale". pp. 75–90. Digital object identifier:10.1002/jts.2490080106. PMID 7712061.
- ↑ Foa E: The Post Traumatic Diagnostic Scale Manual. Minneapolis, NCS, 1995.
- ↑ Brewin; Rose, S; Andrews, B; Green, J; Tata, P; McEvedy, C; Turner, S; Foa, EB (2002). "Brief screening instrument for post traumatic stress disorder". pp. 158–162. PMID 12151288.
- ↑ Foa, E. B., Cashman, L., Jaycox, L. & Perry, K. (1997). The validation of a self-report measure of posttraumatic stress disorder : the Posttraumatic Diagnostic Scale. Psychological Assessment 9, 445–451.
- ↑ Pietrzak RH, Southwick SM (June). "The importance of four-factor emotional numbing and dysphoria models in PTSD". pp. 726–727. Digital object identifier:10.1176/appi.ajp.2009.09010032. PMID 19487403.
- ↑ King DW, Leskin GA, King LA, Weathers FW (June). "Confirmatory factor analysis of the clinician-administered PTSD Scale: Evidence for the dimensionality of posttraumatic stress disorder". pp. 90–96. Digital object identifier:10.1037/1040-3590.10.2.90.
- ↑ Ask E, Mark S (Sep). "The structure of PTSD symptoms: A test of alternative models using confirmatory factor analysis". pp. 299–313. Digital object identifier:10.1348/014466506X171540. PMID 17535523.
- ↑ Palmieri PA, Weathers FW, Difede J, King DW (May). "Confirmatory factor analysis of the PTSD Checklist and the Clinician-Administered PTSD Scale in disaster workers exposed to the World Trade Center Ground Zero". pp. 329–341. Digital object identifier:10.1037/0021-843X.116.2.329. PMID 17516765.
- ↑ Elhai, J. D., & Palmieri, P. A. (2011). "The factor structure of posttraumatic stress disorder: A literature update, critique of methodology, and agenda for future research". pp. 849–854. Digital object identifier:10.1016/j.janxdis.2011.04.007. PMID 21793239.
- ↑ Yufik, T., & Simms, L. J. (2011). "A meta-analytic investigation of the structure of posttraumatic stress disorder symptoms". pp. 764–776. Digital object identifier:10.1037/a0020981. PMID 21090877.
- ↑ 96.0 96.1 "The ICD-10 Classification of Mental and Behavioural Disorders". World Health Organization. pp. 120–121. http://www.who.int/classifications/icd/en/bluebook.pdf.
- ↑ 97.0 97.1 97.2 97.3 97.4 Feldner MT, Monson CM, Friedman MJ (2007). "A critical analysis of approaches to targeted PTSD prevention: current status and theoretically derived future directions". pp. 80–116. Digital object identifier:10.1177/0145445506295057. PMID 17179532.
- ↑ Carlier, IVE; Lamberts RD; van Uchelen AJ; Gersons BPR (1998). "Disaster-related post-traumatic stress in police officers: A field study of the impact of debriefing". pp. 143–8. Digital object identifier:10.1002/(SICI)1099-1700(199807)14:3<143::AID-SMI770>3.0.CO;2-S. http://doi.apa.org/?uid=1998-10258-001.
- ↑ Mayou RA, Ehlers A, Hobbs M (2000). "Psychological debriefing for road traffic accident victims. Three-year follow-up of a randomised controlled trial". pp. 589–93. Digital object identifier:10.1192/bjp.176.6.589. PMID 10974967.
- ↑ Roberts NP, Kitchiner NJ, Kenardy J, Bisson JI (2009). "Cochrane Database of Systematic Reviews". In Roberts, Neil P. Cochrane Database of Systematic Reviews. Digital object identifier:10.1002/14651858.CD006869.pub2. http://www2.cochrane.org/reviews/en/ab006869.html. Retrieved April 27, 2011.
- ↑ Assessment and Management of Conditions Specifically Related to Stress. Geneva: World Health Organization. 2013. ISBN 978 92 4 150593 2. http://apps.who.int/iris/bitstream/10665/85623/1/9789241505932_eng.pdf.
- ↑ 102.0 102.1 102.2 Delahanty DL (2011). "Toward the predeployment detection of risk for PTSD". pp. 9. Digital object identifier:10.1176/appi.ajp.2010.10101519.
- ↑ van Zuiden M, Geuze E, Maas M, Vermetten E, Heijnen CJ, Kavelaars (2009). "Deployment-related severe fatigue with depressive symptoms is associated with increased glucocorticoid binding to peripheral blood mono-nuclear cells". pp. 1132–1139. Digital object identifier:10.1016/j.bbi.2009.07.004. PMID 19635550.
- ↑ 104.0 104.1 Resnik H, Acierno R, Kilpatrick DG, Jager, N (1999). "Prevention of post-rape psychopathology: Preliminary findings of a controlled acute rape treatment study". pp. 359–370. Digital object identifier:10.1016/S0887-6185(99)00010-9. PMID 10504107.
- ↑ van Emmerik, A.A.P., Kamphuis, J.H., et al. (2002). "Single session debriefing after psychological trauma: a meta-analysis". The Lancet 360: 766-771.
- ↑ Cochrane summary on psychological debriefing
- ↑ Cochrane summary on multiple session early psychological interventions for post-traumatic stress disorder
- ↑ American Psychological Association on psychological debriefing
- ↑ Khoshnu, E (October 2006). "Clonidine for Treatment of PTSD". p. 22. Digital object identifier:10.1016/S0270-6644(06)71796-9. http://www.clinicalpsychiatrynews.com/article/S0270-6644%2806%2971796-9/fulltext. Retrieved 9 February 2010.
- ↑ 110.0 110.1 Pitman RK, Sanders KM, Zusman RM, et al. (2002). "Pilot study of secondary prevention of posttraumatic stress disorder with propranolol". pp. 189–92. Digital object identifier:10.1016/S0006-3223(01)01279-3. PMID 11822998.
- ↑ Schelling G, Roozendaal B, Krauseneck T, Schmoelz M, DE Quervain D, Briegel J. (2006). "Efficacy of hydrocortisone in preventing posttraumatic stress disorder following critical illness and major surgery". pp. 46–53. Digital object identifier:10.1196/annals.1364.005. PMID 16891561.
- ↑ Weis F, Kilger E, Roozendaal B, de Quervain DJ, Lamm P, Schmidt M, Schmölz M, Briegel J, Schelling G. (2006). "Stress doses of hydrocortisone reduce chronic stress symptoms and improve health-related quality of life in high-risk patients after cardiac surgery: a randomized study". pp. 277–282. Digital object identifier:10.1016/j.jtcvs.2005.07.063. PMID 16434254.
- ↑ Schelling G, Kilger E, Roozendaal B, de Quervain DJ, Briegel J, Dagge A, Rothenhäusler HB, Krauseneck T, Nollert G, Kapfhammer HP. (2004). "Stress doses of hydrocortisone, traumatic memories, and symptoms of posttraumatic stress disorder in patients after cardiac surgery: a randomized study". pp. 627–633. Digital object identifier:10.1016/j.biopsych.2003.09.014. PMID 15013832.
- ↑ Foa 1997.
- ↑ Cahill, S. P., & Foa, E. B. (2004). A glass half empty or half full? Where we are and directions for future research in the treatment of PTSD. In S. Taylor (ed.), Advances in the Treatment of Posttraumatic Stress Disorder: Cognitive-behavioral perspectives (pp. 267-313) New York: Springer.
- ↑ Brom D, Kleber RJ, Defares PB (October 1989). "Brief psychotherapy for posttraumatic stress disorders". pp. 607–12. Digital object identifier:10.1037/0022-006X.57.5.607. PMID 2571625. http://content.apa.org/journals/ccp/57/5/607.
- ↑ Ehlers A, Bisson J, Clark DM, et al. (March 2010). "Do all psychological treatments really work the same in posttraumatic stress disorder?". pp. 269–76. Digital object identifier:10.1016/j.cpr.2009.12.001. PMC 2852651. PMID 20051310.
- ↑ Bisson JI, Ehlers A, Matthews R, Pilling S, Richards D, Turner S (2007). "Psychological treatments for chronic post-traumatic stress disorder. Systematic review and meta-analysis". pp. 97–104. Digital object identifier:10.1192/bjp.bp.106.021402. PMID 17267924. http://bjp.rcpsych.org/cgi/content/full/190/2/97.
- ↑ Seidler GH, Wagner FE (2006). "Comparing the efficacy of EMDR and trauma-focused cognitive-behavioral therapy in the treatment of PTSD: a meta-analytic study". pp. 1515–22. Digital object identifier:10.1017/S0033291706007963. PMID 16740177.
- ↑ Hassija, C.M. & Gray, M.J. (2007). Behavioral Interventions for Trauma and Posttraumatic Stress Disorder. International Journal of Behavioral Consultation and Therapy 3 (2166-175. BAO
- ↑ Mulick, P.S., Landes, S. & Kanter, J.W. (2005) Contextual Behavior Therapies in the Treatment of PTSD: A Review. International Journal of Behavioral Consultation and Therapy 1 (3 223-228 [4]
- ↑ Hassija, C.M. & Gray, M.J. (2007). Behavioral Interventions for Trauma and Posttraumatic Stress Disorder. International Journal of Behavioral Consultation and Therapy 3 (2 166-175. [5]
- ↑ Mulick, P.S., and Naugle, A.E. (2009). Behavioral Activation in the Treatment of Comorbid Posttraumatic Stress Disorder and Major Depressive Disorder. International Journal of Behavioral Consultation and Therapy 5 (2 330-339. [6]
- ↑ Grohol, JM. "What is Exposure Therapy?". http://psychcentral.com/lib/2009/what-is-exposure-therapy/. Retrieved 2010-07-14.
- ↑ Joseph, JS; Gray, M.J. (2008). BAO "Exposure Therapy for Posttraumatic Stress Disorder". pp. 69–80. http://www.baojournal.com BAO. Retrieved 2010-05-10.
- ↑ Ursano RJ, Bell C, Eth S, et al. (November 2004). "Practice guideline for the treatment of patients with acute stress disorder and posttraumatic stress disorder". pp. 3–31. PMID 15617511.
- ↑ Committee on Treatment of Posttraumatic Stress Disorder, Institute of Medicine: Treatment of Posttraumatic Stress Disorder: An Assessment of the Evidence. Washington, D.C.: National Academies Press, 2008 ISBN 0-309-10926-4.
- ↑ "Prolonged Exposure Therapy". 2009-09-29. http://www.ptsd.va.gov/public/pages/prolonged-exposure-therapy.asp. Retrieved 2010-07-14.
- ↑ Karlin B. E., Ruzek J. I. Chard, Eftekhari A., Monson C. M., Hembree E. A., Resick P. A., Foa E. B. (2010). "Dissemination of evidence-based psychological treatments for posttraumatic stress disorder in the Veterans Health Administration". pp. 663–673. Digital object identifier:10.1002/jts.20588. PMID 21171126.
- ↑ 130.0 130.1 Shapiro, Francine (April 1989). "Efficacy of the eye movement desensitization procedure in the treatment of traumatic memories". pp. 199–223. Digital object identifier:10.1002/jts.2490020207.
- ↑ Shapiro, F; Maxfield, L (2002 Aug). "Eye Movement Desensitization and Reprocessing (EMDR): information processing in the treatment of trauma.". pp. 933–46. Digital object identifier:10.1002/jclp.10068. PMID 12115716.
- ↑ 132.0 132.1 The Management of Post-Traumatic Stress Working Group (2010). "VA/DoD clinical practice guideline for management of post-traumatic stress". Department of Veterans Affairs, Department of Defense. p. Version 2.0. http://www.healthquality.va.gov/Post_Traumatic_Stress_Disorder_PTSD.asp. Retrieved 2 June 2013.
- ↑ 133.0 133.1 133.2 Gillies, Donna; Taylor F, Gray C, O'Brien L, D'Abrew N (2012). "Psychological therapies for the treatment of post‐traumatic stress disorder in children and adolescents". In Gillies, Donna. Digital object identifier:10.1002/14651858.CD006726.pub2. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0050297/.
- ↑ 134.0 134.1 Jeffries, FW; Davis, P (2013 May). "What is the role of eye movements in eye movement desensitization and reprocessing (EMDR) for post-traumatic stress disorder (PTSD)? a review.". pp. 290–300. Digital object identifier:10.1017/S1352465812000793. PMID 23102050.
- ↑ 135.0 135.1 135.2 135.3 135.4 135.5 Jonas, Daniel E; Cusack K, Forneris CA et al (April 2013). "Psychological and pharmacological treatments for adults with posttraumatic stress disorder (PTSD)". Agency for Healthcare Quality and Research. p. Comparative Effectiveness Reviews, No 92. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0055845/. Retrieved 2 June 2013. Cite error: Invalid
<ref>tag; name "AHRQtreat92" defined multiple times with different content - ↑ Weissman MM, Markowitz JC, Klerman GL: Clinician’s Quick Guide to Interpersonal Psychotherapy. New York: Oxford University Press, 2007.
- ↑ Bleiberg KL, Markowitz JC (January 2005). "A pilot study of interpersonal psychotherapy for posttraumatic stress disorder". pp. 181–3. Digital object identifier:10.1176/appi.ajp.162.1.181. PMID 15625219.
- ↑ http://www.columbiatrauma.org/
- ↑ Markowitz JC, Milrod B, Bleiberg K, Marshall RD (March 2009). "Interpersonal factors in understanding and treating posttraumatic stress disorder". pp. 133–40. Digital object identifier:10.1097/01.pra.0000348366.34419.28. PMC 2852131. PMID 19339847.
- ↑ Markowitz JC: IPT and PTSD. Depress Anxiety. 2010 Oct;27(10) 879-81.
- ↑ Maxmen, J. S.; Ward, N. G. (1995). Essential psychopathology and its treatment, 2nd ed., revised for DSM-IV (second ed.). New York: W. W. Norton. p. 280. ISBN 0-393-70173-5.
- ↑ 142.0 142.1 Maxmen, J. S.; Ward, N. G. (2002). Psychotropic drugs: fast facts (third ed.). New York: W. W. Norton. p. 346. ISBN 0-393-70301-0.
- ↑ Krystal, John H; Alexander Neumeister (2009). "Noradrenergic and serotonergic mechansims in the neurobiology of posttraumatic stress disorder and resilience". pp. 13–23. Digital object identifier:10.1016/j.brainres.2009.03.044. PMC 2761677. PMID 19332037.
- ↑ Bisson, Jonathan I (2008). "Pharmacological treatment to prevent and treat post-traumatic stress disorder". pp. 104–eoa.
- ↑ 145.0 145.1 Berger, W.; Mendlowicz, MV.; Marques-Portella, C.; Kinrys, G.; Fontenelle, LF.; Marmar, CR.; Figueira, I. (Mar 2009). "Pharmacologic alternatives to antidepressants in posttraumatic stress disorder: a systematic review". pp. 169–80. Digital object identifier:10.1016/j.pnpbp.2008.12.004. PMC 2720612. PMID 19141307.
- ↑ Cooper, J.; Carty, J.; Creamer, M. (Aug 2005). "Pharmacotherapy for posttraumatic stress disorder: empirical review and clinical recommendations". pp. 674–82. Digital object identifier:10.1111/j.1440-1614.2005.01651.x. PMID 16050921.
- ↑ Yehuda R (2000). "Biology of posttraumatic stress disorder". pp. 14–21. PMID 10795605.
- ↑ 148.0 148.1 148.2 148.3 148.4 148.5 148.6 Maxmen, J. S.; Ward, N. G. (2002). Psychotropic drugs: fast facts (third ed.). New York: W. W. Norton. p. 347. ISBN 0-393-70301-0.
- ↑ Marshall RD, Beebe KL, Oldham M, Zaninelli R (December 2001). "Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study". pp. 1982–8. Digital object identifier:10.1176/appi.ajp.158.12.1982. PMID 11729013. http://ajp.psychiatryonline.org/cgi/pmidlookup?view=long&pmid=11729013.
- ↑ Brady K, Pearlstein T, Asnis GM, et al. (April 2000). "Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial". pp. 1837–44. Digital object identifier:10.1001/jama.283.14.1837. PMID 10770145. http://jama.ama-assn.org/cgi/pmidlookup?view=long&pmid=10770145.
- ↑ Davidson JR, Rothbaum BO, van der Kolk BA, Sikes CR, Farfel GM (May 2001). "Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder". pp. 485–92. Digital object identifier:10.1001/archpsyc.58.5.485. PMID 11343529. http://archpsyc.ama-assn.org/cgi/pmidlookup?view=long&pmid=11343529.
- ↑ Maxmen, J. S.; Ward, N. G. (1995). Essential psychopathology and its treatment, 2nd ed., revised for DSM-IV (second ed.). New York: W. W. Norton. p. 104. ISBN 0-393-70173-5.
- ↑ Maxmen, J. S.; Ward, N. G. (1995). Essential psychopathology and its treatment, 2nd ed., revised for DSM-IV (second ed.). New York: W. W. Norton. p. 175. ISBN 0-393-70173-5.
- ↑ 154.0 154.1 154.2 154.3 154.4 154.5 Maxmen, J. S.; Ward, N. G. (2002). Psychotropic drugs: fast facts (third ed.). New York: W. W. Norton. p. 349. ISBN 0-393-70301-0.
- ↑ 155.0 155.1 Lacy CF, Armstrong LL et al. (2008). Drug Information Handbook. Lexi-Comp. pp. 260, 934.
- ↑ "Lamotrigine FAQ". http://www.psycom.net/depression.central.lamotrigine.html. Retrieved 2007-05-01.
- ↑ SSRIs versus Non-SSRIs in Post-traumatic Stress Disorder, Department of Psychiatry and Behavioral Sciences, Montefiore Medical Center, Albert Einstein College of Medicine.
- ↑ Hertzberg MA, Butterfield MI, Feldman ME, et al. (May 1999). "A preliminary study of lamotrigine for the treatment of posttraumatic stress disorder". pp. 1226–9. Digital object identifier:10.1016/S0006-3223(99)00011-6. PMID 10331117. http://linkinghub.elsevier.com/retrieve/pii/S0006-3223(99)00011-6.
- ↑ 159.0 159.1 159.2 Kapfhammer, HP. (Dec 2008). "[Therapeutic possibilities after traumatic experiences]". pp. 532–45. PMID 19011595.
- ↑ http://www.annals-general-psychiatry.com/content/5/S1/S159
- ↑ Maxmen, J. S.; Ward, N. G. (1995). Essential psychopathology and its treatment, 2nd ed., revised for DSM-IV (second ed.). New York: W. W. Norton. p. 95. ISBN 0-393-70173-5.
- ↑ Jain S, Greenbaum MA, Rosen C (February 2012). "Concordance between psychotropic prescribing for veterans with PTSD and clinical practice guidelines". pp. 154–60. Digital object identifier:10.1176/appi.ps.201100199. PMID 22302333.
- ↑ 163.0 163.1 Reist, C (2005). Post-traumatic Stress Disorder. Compendia, Build ID: F000005, published by Epocrates.com
- ↑ Auxéméry Y (October 2012). "[Posttraumatic stress disorder (PTSD) as a consequence of the interaction between an individual genetic susceptibility, a traumatogenic event and a social context]" (in French). pp. 373–80. Digital object identifier:10.1016/j.encep.2011.12.003. PMID 23062450.
- ↑ Martényi, F. (Mar 2005). "[Three paradigms in the treatment of posttraumatic stress disorder]". pp. 11–21. PMID 16167463.
- ↑ Cohen H, Matar MA, Buskila D, Kaplan Z, Zohar J. (2008). "Early post-stressor intervention with high-dose corticosterone attenuates posttraumatic stress response in an animal model of posttraumatic stress disorder". pp. 708–717. Digital object identifier:10.1016/j.biopsych.2008.05.025. PMID 18635156.
- ↑ Sapolsky RM, Romero LM, Munck AU. (2000). "How do glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparative actions". pp. 55–89. Digital object identifier:10.1210/er.21.1.55. PMID 10696570.
- ↑ "Study of 3,4-Methylenedioxymethamphetamine-Assisted Psychotherapy in People With Posttraumatic Stress Disorder". ClinicalTrials.gov. U.S. National Institutes of Health. February 2009. http://clinicaltrials.gov/ct2/show/NCT00353938. Retrieved on June 17, 2009.
- ↑ "Randomized Placebo-Controlled Study of MDMA-Assisted Psychotherapy in People With PTSD - Israel". ClinicalTrials.gov. U.S. National Institutes of Health. February 2009. http://clinicaltrials.gov/ct2/show/NCT00402298. Retrieved on June 17, 2009.
- ↑ 170.0 170.1 Maxmen, J. S.; Ward, N. G. (2002). Psychotropic drugs: fast facts (third ed.). New York: W. W. Norton. pp. 347–349. ISBN 0-393-70301-0.
- ↑ 171.0 171.1 Lawrence, Sue; De Silva M, Henley R (2010). "Sports and games for post-traumatic stress disorder (PTSD)". In Lawrence, Sue. Digital object identifier:10.1002/14651858.CD007171.pub2. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0014346/.
- ↑ Jankowski, K. "PTSD and physical health". Information on trauma and PTSD for professionals, National Center for PTSD. U.S. Department of Veterans Affairs. http://www.ptsd.va.gov/professional/pages/ptsd-physical-health.asp. Retrieved 8 June 2013.
- ↑ U.S. Department of Veterans Affairs. "Lifestyle Changes Recommended for PTSD Patients". Information on trauma and PTSD for veterans, general public and family from the National Center for PTSD. U.S. Department of Veterans Affairs. http://www.ptsd.va.gov/public/pages/coping-ptsd-lifestyle-changes.asp. Retrieved 8 June 2013.
- ↑ Liedl, Alexandra; Müller, Julia; Morina, Naser; Karl, Anke; Denke, Claudia; Knaevelsrud, Christine (1 February 2011). "Physical Activity within a CBT Intervention Improves Coping with Pain in Traumatized Refugees: Results of a Randomized Controlled Design". pp. 234–245. Digital object identifier:10.1111/j.1526-4637.2010.01040.x. PMID 21223501.
- ↑ Rosenbaum, S; Nguyen, D; Lenehan, T; Tiedemann, A; van der Ploeg, HP; Sherrington, C (2011 Jul 22). "Exercise augmentation compared to usual care for post traumatic stress disorder: a randomised controlled trial (the REAP study: Randomised Exercise Augmentation for PTSD).". pp. 115. Digital object identifier:10.1186/1471-244X-11-115. PMC 3151207. PMID 21777477.
- ↑ Neylan, TC. "Integrative Exercise for Post-Deployment Stress". ClinicalTrials.gov Identifier: NCT01674244. US National Institutes of Health (NIH). http://clinicaltrials.gov/ct2/show/NCT01674244. Retrieved 8 June 2013.
- ↑ Smits, J. "Maximizing Treatment Outcome and Examining Sleep in Post-traumatic Stress Disorder (PTSD)". ClinicalTrials.gov Identifier: NCT01199107. US National Institutes of Health (NIH). http://clinicaltrials.gov/ct2/show/NCT01199107. Retrieved 8 June 2013.
- ↑ 178.0 178.1 178.2 178.3 Wethington, Holly R.; Hahn, Robert A.; Fuqua-Whitley, Dawna S.; Sipe, Theresa Ann; Crosby, Alex E.; Johnson, Robert L.; Liberman, Akiva M.; Mościcki, Eve; Price, LeShawndra N.; Tuma, Farris K.; Kalra, Geetika; Chattopadhyay, Sajal K. (31 August 2008). "The Effectiveness of Interventions to Reduce Psychological Harm from Traumatic Events Among Children and Adolescents". pp. 287–313. Digital object identifier:10.1016/j.amepre.2008.06.024. PMID 18692745. http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0026074.
- ↑ Fletcher KE; Barkley, Russell A. (2003). "7". In Mash, Eric J.. Child psychopathology (2nd ed.). New York: Guilford Press. pp. 330–371. ISBN 1-57230-609-2.
- ↑ Hamblen, J; Barnett, E (20). "PTSD in children and adolescents". VA National Center for Posttraumatic Stress Disorder. http://www.ptsd.va.gov/professional/pages/ptsd_in_children_and_adolescents_overview_for_professionals.asp. Retrieved 10 June 2013.
- ↑ "Mortality and Burden of Disease Estimates for WHO Member States in 2004". World Health Organization. http://www.who.int/entity/healthinfo/global_burden_disease/gbddeathdalycountryestimates2004.xls.
- ↑ Brunet A, Akerib V, Birmes P (2007). "Don't throw out the baby with the bathwater (PTSD is not overdiagnosed)" (PDF). pp. 501–2; discussion 503. PMID 17955912. http://publications.cpa-apc.org/media.php?mid=490. Retrieved 2008-03-12.
- ↑ 183.0 183.1 List of countries by population
- ↑ 184.0 184.1 "Mortality and Burden of Disease Estimates for WHO Member States: Persons, all ages (2004)" (xls). World Health Organization. 2004. http://www.who.int/entity/healthinfo/global_burden_disease/gbddeathdalycountryestimates2004.xls. Retrieved 2009-11-12.
- ↑ 185.0 185.1 "Mortality and Burden of Disease Estimates for WHO Member States: Females, all ages (2004)" (xls). World Health Organization. 2004. http://www.who.int/entity/healthinfo/global_burden_disease/gbddeathdalycountryestimates_female_2004.xls. Retrieved 2009-11-12.
- ↑ 186.0 186.1 "Mortality and Burden of Disease Estimates for WHO Member States: Males, all ages (2004)" (xls). World Health Organization. 2004. http://www.who.int/entity/healthinfo/global_burden_disease/gbddeathdalycountryestimates_male_2004.xls. Retrieved 2009-11-12.
- ↑ Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB (December 1995). "Posttraumatic stress disorder in the National Comorbidity Survey". pp. 1048–60. Digital object identifier:10.1001/archpsyc.1995.03950240066012. PMID 7492257.
- ↑ Sher, Leo (2010). "Neurobiology of suicidal behavior in post-traumatic stress disorder". pp. 1233–1235.
- ↑ Mintz, S. (2007) The War's Costs. Digital History.
- ↑ "Psychological Costs of War: Military Combat and Mental Health". journalistsresource.org. http://journalistsresource.org/studies/government/federalstate/psychological-costs-war-military-combat-mental-health/.
- ↑ Department of Veterans Affairs Office of Inspector General (May 19, 2005). "Review of State Variances in VA Disability Compensation Payments". Washington, DC: Department of Veterans Affairs Office of Inspector General. http://www.va.gov/oig/52/reports/2005/VAOIG-05-00765-137.pdf. Retrieved 2011-09-03.
- ↑ Hedenko, William. "The Relationship Between PTSD and Suicide". http://www.ptsd.va.gov/professional/pages/ptsd-suicide.asp. Retrieved 3 November 2011.
- ↑ Secretary Nicholson (2005-11-10). "No Across-the-Board Review of PTSD Cases". The Department of Veterans Affairs.; United States Department of Veteran Affairs.
- ↑ "Marine Corps Offers Yoga, Massages to Marriages Strained by War". Fox News. 2008-04-02. http://www.foxnews.com/story/0,2933,344991,00.html. Retrieved 2008-04-03.
- ↑ Welcome to the American Legion Online
- ↑ "Sierra Club Military Families and Veterans Initiative". http://sierraclub.typepad.com/military/. Retrieved 2012-07-26.
- ↑ 197.0 197.1 Reed McManus (2011-08). "A Missing Peace - Can wilderness adventure repair the ravages of war?". Sierra Magazine - Sierra Club. http://www.sierraclub.org/sierra/201107/a-missing-peace.aspx. Retrieved 2012-07-26.
- ↑ "Military Families and Veterans Initiative: Grizzly Tracking in Montana for Veterans, Service Members, and Families". http://sierraclub.typepad.com/military/2012/06/grizzly-tracking-in-montana-for-veterans-service-members-and-families.html. Retrieved 2012-07-26.
- ↑ Dixon, Laura (February 28, 2009). "Lance Corporal Johnson Beharry accuses Government of neglecting soldiers". London: Times Online. http://www.timesonline.co.uk/tol/news/politics/article5819059.ece. Retrieved 2009-08-29.
- ↑ Hickley, Matthew; Hope, Jenny (2009-03-02). "British troops in Afghanistan face mental health timebomb 'on the scale of Vietnam' | Mail Online". London: Dailymail.co.uk. http://www.dailymail.co.uk/news/article-1158350/Troops-face-mental-trauma-scale-Vietnam.html. Retrieved 2009-08-29.
- ↑ "UK | Full interview: L/Cpl Johnson Beharry". BBC News. 2009-02-28. http://news.bbc.co.uk/1/hi/uk/7916852.stm. Retrieved 2009-08-29.
- ↑ The Operational Stress Injury Social Support (OSISS) Program for Canadian Veterans. See also "Evaluation of the OSISS Peer Support Network," Dept. of National Defence and Veterans Affairs Canada, January 2005.
- ↑ Heber, A., Grenier, S., Richardson, D., Darte, K. (2006). "Combining Clinical Treatment and Peer Support: A Unique Approach to Overcoming Stigma and Delivering Care." In Human Dimensions in Military Operations – Military Leaders’ Strategies for Addressing Stress and Psychological Support; Neuilly-sur-Seine, France, Canadian Department Of National Defence.
- ↑ Richardson, J. D., K. Darte, et al. (2008). "Operational Stress Injury Social Support: a Canadian innovation in professional peer support." Can Mil J 9: 57-64.
- ↑ "The New Veterans Charter for CF Veterans and their Families". Vac-Acc.Gc.Ca. 2006-07-12. http://www.vac-acc.gc.ca/clients/sub.cfm?source=Forces/nvc&CFID=9295860&CFTOKEN=39698927. Retrieved 2009-08-29.
- ↑ Shay, Jonathan Achilles in Vietnam: Combat Trauma and the Undoing of Character, Scribner, 1994; pp. 165-66.
- ↑ World War One – A New Kind of War | Part II, From 14 - 18 Understanding the Great War, by Stéphane Audoin-Rouzeau, Annette Becker
- ↑ 208.0 208.1 208.2 When trauma tips you over: PTSD Part 1 All in the Mind, Australian Broadcasting Commission, 9 October 2004.
- ↑ Andreasen, Nancy C. (Feb 19, 2004). Brave New Brain: Conquering Mental Illness in the Era of the Genome. New York: Oxford University Press. p. 303. ISBN 978-0-19-516728-3.
- ↑ 210.0 210.1 Shalev, Arieh Y.; Yehuda, Rachel; Alexander C. McFarlane (2000). International handbook of human response to trauma. New York: Kluwer Academic/Plenum Press. ISBN 0-306-46095-5.;on-line.
- ↑ "International Statistical Classification of Diseases and Related Health Problems 10th Revision Version for 2007". World Health Organization (UN). 2007. http://en.wikipedia.org/wiki/Posttraumatic_stress_disorder#Terminology. Retrieved October 3, 2011.
External links[]
| Wikimedia Commons has media related to Posttraumatic stress disorder. |
- Posttraumatic stress disorder at DMOZ
- Resources for the public from VA National PTSD Center
- Resources for professionals from VA National PTSD Center
- Post Traumatic Stress Disorder Information Resource from The University of Queensland School of Medicine
- Resources for Parents of Children with PTSD from The Children's Hospital of Philadelphia
The original article can be found at Posttraumatic stress disorder and the edit history here.